

Predictors of virological failure among people living with HIV receiving first line antiretroviral treatment in Myanmar: retrospective cohort analysis
- PMID: 33882962
- PMCID: PMC8059266
- DOI: 10.1186/s12981-021-00336-0
Predictors of virological failure among people living with HIV receiving first line antiretroviral treatment in Myanmar: retrospective cohort analysis
Abstract
Background: Progress toward the global target for 95% virological suppression among those on antiretroviral treatment (ART) is still suboptimal. We describe the viral load (VL) cascade, the incidence of virological failure and associated risk factors among people living with HIV receiving first-line ART in an HIV cohort in Myanmar treated by the Médecins Sans Frontières in collaboration with the Ministry of Health and Sports Myanmar.
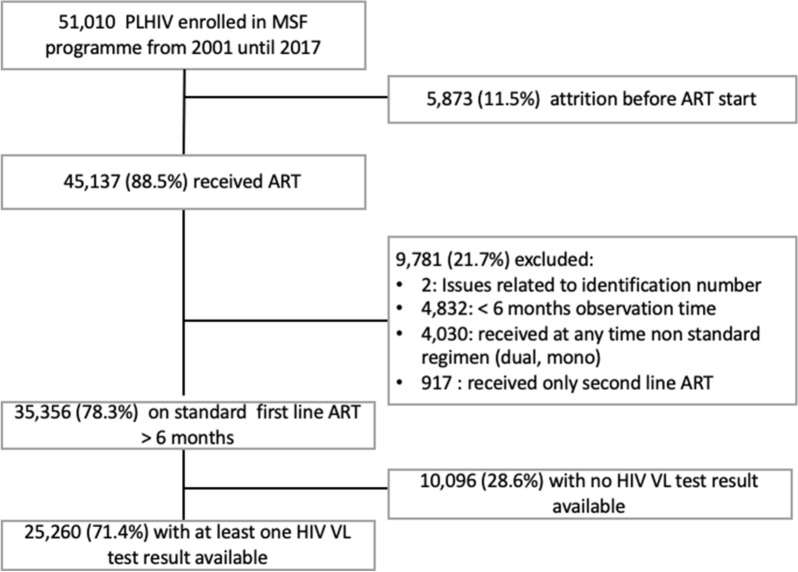
Methods: We conducted a retrospective cohort study, including adult patients with at least one HIV viral load test result and having received of at least 6 months' standard first-line ART. The incidence rate of virological failure (HIV viral load ≥ 1000 copies/mL) was calculated. Multivariable Cox's regression was performed to identify risk factors for virological failure.
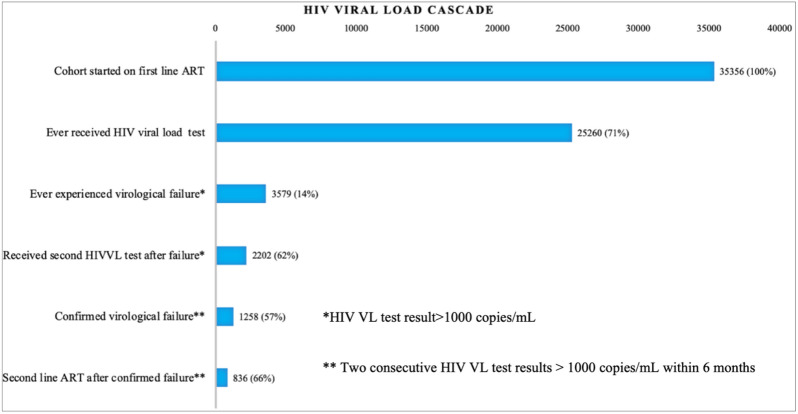
Results: We included 25,260 patients with a median age of 33.1 years (interquartile range, IQR 28.0-39.1) and a median observation time of 5.4 years (IQR 3.7-7.9). Virological failure was documented in 3,579 (14.2%) participants, resulting in an overall incidence rate for failure of 2.5 per 100 person-years of follow-up. Among those who had a follow-up viral load result, 1,258 (57.1%) had confirmed virological failure, of which 836 (66.5%) were switched to second-line treatment. An increased hazard for failure was associated with age ≤ 19 years (adjusted hazard ratio, aHR 1.51; 95% confidence intervals, CI 1.20-1.89; p < 0.001), baseline tuberculosis (aHR 1.39; 95% CI 1.14-1.49; p < 0.001), a history of low-level viremia (aHR 1.60; 95% CI 1.42-1.81; p < 0.001), or a history of loss-to-follow-up (aHR 1.24; 95% CI 1.41-1.52; p = 0.041) and being on the same regimen (aHR 1.37; 95% CI 1.07-1.76; p < 0.001). Cumulative appointment delay was not significantly associated with failure after controlling for covariates.
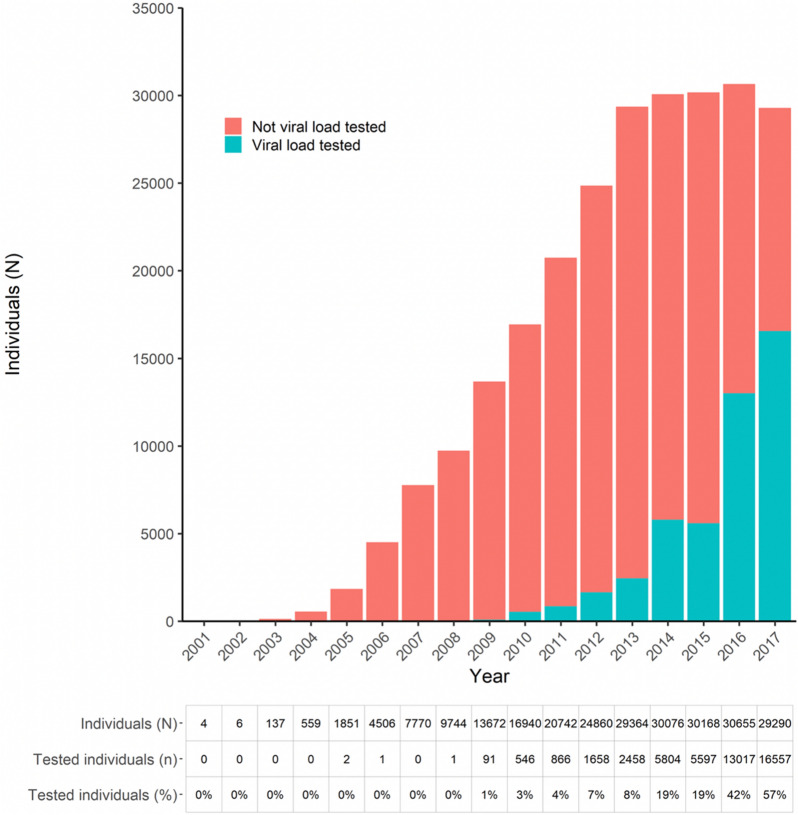
Conclusions: VL monitoring is an important tool to improve programme outcomes, however limited coverage of VL testing and acting on test results hampers its full potential. In our cohort children and adolescents, PLHIV with history of loss-to-follow-up or those with low-viremia are at the highest risk of virological failure and might require more frequent virological monitoring than is currently recommended.
Keywords: First-line antiretroviral treatment; HIV; Lost-to-follow up; Low viremia; Myanmar; Virological failure.
Conflict of interest statement
Authors have no competing interest to declare.
Figures
References
-
- UNAIDS. Fast Track Strategy to end the AIDS epidemic by 2030. [Internet]. 2014. https://www.unaids.org/sites/default/files/media_asset/JC2686_WAD2014rep.... Accessed 20 Jul 2020.
-
- UNAIDS. UNAIDS Data 2019. [Internet]. 2019. https://www.unaids.org/en/resources/documents/2019/2019-UNAIDS-data. Accessed 30 Jul 2020.
-
- Haas AD, Keiser O, Balestre E, Brown S, Bissagnene E, Chimbetete C, et al. Monitoring and switching of first-line antiretroviral therapy in adult treatment cohorts in sub-Saharan Africa: collaborative analysis. The lancet HIV. 2015;2(7):e271–e278. doi: 10.1016/S2352-3018(15)00087-9. - DOI - PMC - PubMed
-
- Kyaw NTT, Harries AD, Kumar AMV, Oo MM, Kyaw KWY, Win T, et al. High rate of virological failure and low rate of switching to second-line treatment among adolescents and adults living with HIV on first-line ART in Myanmar, 2005–2015. PLoS ONE. 2017;12(2):e0171780. doi: 10.1371/journal.pone.0171780. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
