

How can human resources for health interventions contribute to sexual, reproductive, maternal, and newborn healthcare quality across the continuum in low- and lower-middle-income countries? A systematic review
- PMID: 33882968
- PMCID: PMC8061056
- DOI: 10.1186/s12960-021-00601-3
How can human resources for health interventions contribute to sexual, reproductive, maternal, and newborn healthcare quality across the continuum in low- and lower-middle-income countries? A systematic review
Abstract
Background: Well-trained, competent, and motivated human resources for health (HRH) are crucial to delivering quality service provision across the sexual, reproductive, maternal, and newborn health (SRMNH) care continuum to achieve the 2030 Sustainable Development Goals (SDGs) maternal and neonatal health targets. This review aimed to identify HRH interventions to support lay and/or skilled personnel to improve SRMNH care quality along the continuum in low- and lower-middle-income countries (LLMICs).
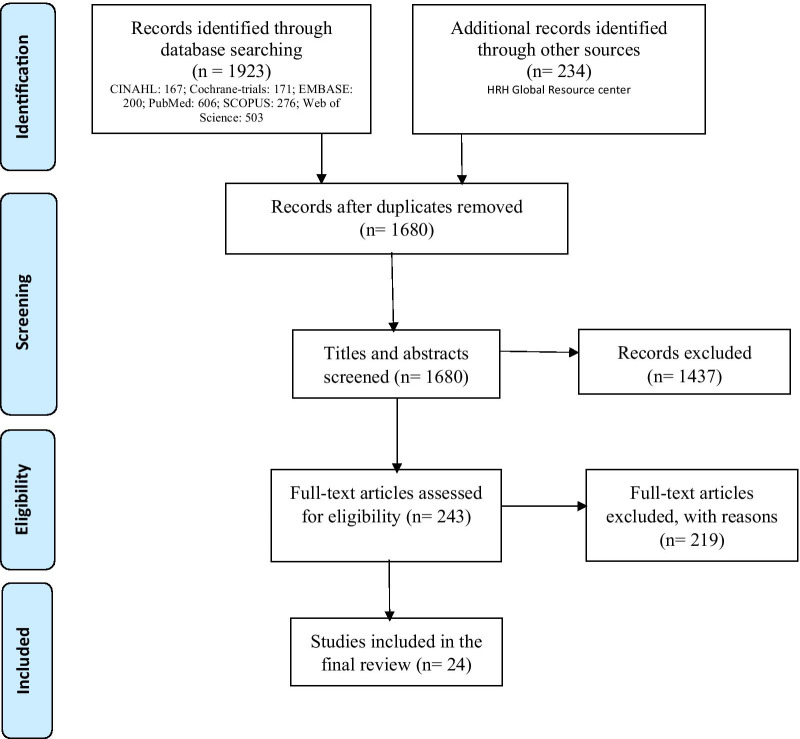
Methods: A structured search of CINAHL, Cochrane Library/trials, EMBASE, PubMed, SCOPUS, Web of Science, and HRH Global Resource Centre databases was undertaken, guided by the PRISMA framework. The inclusion criteria sought to identify papers with a focus on 1. HRH management, leadership, partnership, finance, education, and/or policy interventions; 2. HRH interventions' impact on two or more quality SRMNH care packages across the continuum from preconception to pregnancy, intrapartum and postnatal care; 3. Skilled and/or lay personnel; and 4. Reported primary research in English from LLMICs. A deductive qualitative content analysis was employed using the World Health Organization-HRH action framework.
Results: Out of identified 2157 studies, 24 intervention studies were included in the review. Studies where ≥ 4 HRH interventions had been combined to target various healthcare system components, were more effective than those implementing ≤ 3 HRH interventions. In primary care, HRH interventions involving skilled and lay personnel were more productive than those involving either skilled or lay personnel alone. Results-based financing (RBF) and its policy improved the quality of targeted maternity services but had no impact on client satisfaction. Local budgeting, administration, and policy to deliver financial incentives to health workers and improve operational activities were more efficacious than donor-driven initiatives. Community-based recruitment, training, deployment, empowerment, supportive supervision, access to m-Health technology, and modest financial and non-financial incentives for community health workers (CHWs) improved the quality of care continuum. Skills-based, regular, short, focused, onsite, and clinical simulation, and/or mobile phone-assisted in-service training of skilled personnel were more productive than knowledge-based, irregular, and donor-funded training. Facility-based maternal and perinatal death reviews, coupled with training and certification of skilled personnel, positively affected SRMNH care quality across the continuum. Preconception care, an essential component of the SRMNH care continuum, lacks studies and services in LLMICs.
Conclusions: We recommend maternal and perinatal death audits in all health facilities; respectful, woman-centered care as a critical criterion of RBF initiatives; local administration of health worker allowances and incentives; and integration of CHWs into the healthcare system. There is an urgent need to include preconception care in the SRMNH care continuum and studies in LLMICs.
Keywords: And newborn health; Deductive qualitative content analysis; Human resources for health intervention; Lay personnel; Low- and lower-middle-income countries; Maternal; Quality of care; Reproductive; Sexual; Skilled personnel; The continuum of care.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Systematic review on human resources for health interventions to improve maternal health outcomes: evidence from low- and middle-income countries.Hum Resour Health. 2016 Mar 12;14:10. doi: 10.1186/s12960-016-0106-y. Hum Resour Health. 2016. PMID: 26971317 Free PMC article.
-
Effects of consumers and health providers working in partnership on health services planning, delivery and evaluation.Cochrane Database Syst Rev. 2021 Sep 15;9(9):CD013373. doi: 10.1002/14651858.CD013373.pub2. Cochrane Database Syst Rev. 2021. PMID: 34523117 Free PMC article.
-
Training and expertise in undertaking assisted vaginal delivery (AVD): a mixed methods systematic review of practitioners views and experiences.Reprod Health. 2021 May 5;18(1):92. doi: 10.1186/s12978-021-01146-3. Reprod Health. 2021. PMID: 33952309 Free PMC article.
-
Support for healthy breastfeeding mothers with healthy term babies.Cochrane Database Syst Rev. 2022 Oct 25;10(10):CD001141. doi: 10.1002/14651858.CD001141.pub6. Cochrane Database Syst Rev. 2022. PMID: 36282618 Free PMC article.
-
Population-based interventions for reducing sexually transmitted infections, including HIV infection.Cochrane Database Syst Rev. 2004;(2):CD001220. doi: 10.1002/14651858.CD001220.pub2. Cochrane Database Syst Rev. 2004. Update in: Cochrane Database Syst Rev. 2011 Mar 16;(3):CD001220. doi: 10.1002/14651858.CD001220.pub3. PMID: 15106156 Updated.
Cited by
-
Building leadership and managerial capacity for maternal and newborn health services.BMC Health Serv Res. 2022 Sep 7;22(1):1129. doi: 10.1186/s12913-022-08448-7. BMC Health Serv Res. 2022. PMID: 36071415 Free PMC article.
-
Effective coverage for reproductive, maternal, neonatal and newborn health: an analysis of geographical and socioeconomic inequalities in 39 low- and middle-income countries.BMJ Glob Health. 2025 Feb 17;10(2):e016549. doi: 10.1136/bmjgh-2024-016549. BMJ Glob Health. 2025. PMID: 39961692 Free PMC article.
-
Women's utilisation of quality antenatal care, intrapartum care and postnatal care services in Ethiopia: a population-based study using the demographic and health survey data.BMC Public Health. 2023 Jun 19;23(1):1174. doi: 10.1186/s12889-023-15938-8. BMC Public Health. 2023. PMID: 37337146 Free PMC article.
-
Essential components of postnatal care - a systematic literature review and development of signal functions to guide monitoring and evaluation.BMC Pregnancy Childbirth. 2022 May 28;22(1):448. doi: 10.1186/s12884-022-04752-6. BMC Pregnancy Childbirth. 2022. PMID: 35643432 Free PMC article.
-
Optimal Strategies for Screening Common Birth Defects in Children of Low- and Middle-Income Countries: A Systematic Review.Neonatology. 2025;122(Suppl 1):224-244. doi: 10.1159/000541697. Epub 2024 Oct 25. Neonatology. 2025. PMID: 39462499 Free PMC article.
References
-
- World Health Organization: Maternal health. https://www.whoint/health-topics/maternal-health#tab=tab_1 accessed 27 March 2021.
-
- World Health Organization. https://www.whoint/health-topics/maternal-health#tab=tab_2 accessed 27 March 2021. Maternal Health.
-
- Kruk ME, Gage AD, Arsenault C, Jordan K, Leslie HH, Roder-DeWan S, Adeyi O, Barker P, Daelmans B, Doubova SV. High-quality health systems in the Sustainable Development Goals era: time for a revolution. Lancet Glob Health. 2018;6(11):e1196–e1252. doi: 10.1016/S2214-109X(18)30386-3. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
