

Severe acute myopathy following SARS-CoV-2 infection: a case report and review of recent literature
- PMID: 33883014
- PMCID: PMC8058144
- DOI: 10.1186/s13395-021-00266-5
Severe acute myopathy following SARS-CoV-2 infection: a case report and review of recent literature
Abstract
Background: SARS-CoV2 virus could be potentially myopathic. Serum creatinine phosphokinase (CPK) is frequently found elevated in severe SARS-CoV2 infection, which indicates skeletal muscle damage precipitating limb weakness or even ventilatory failure.
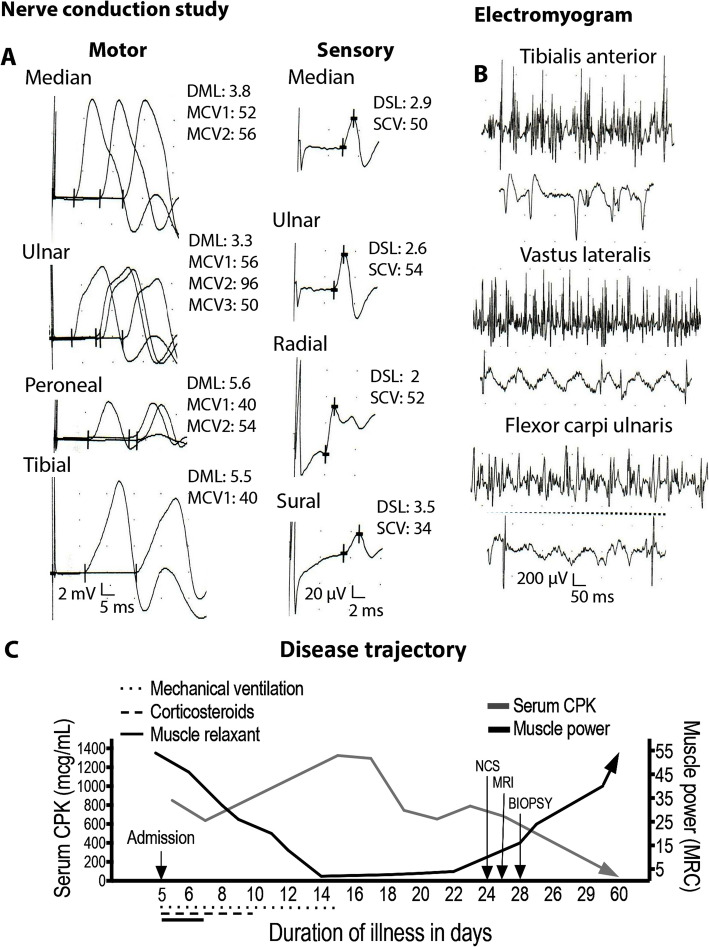
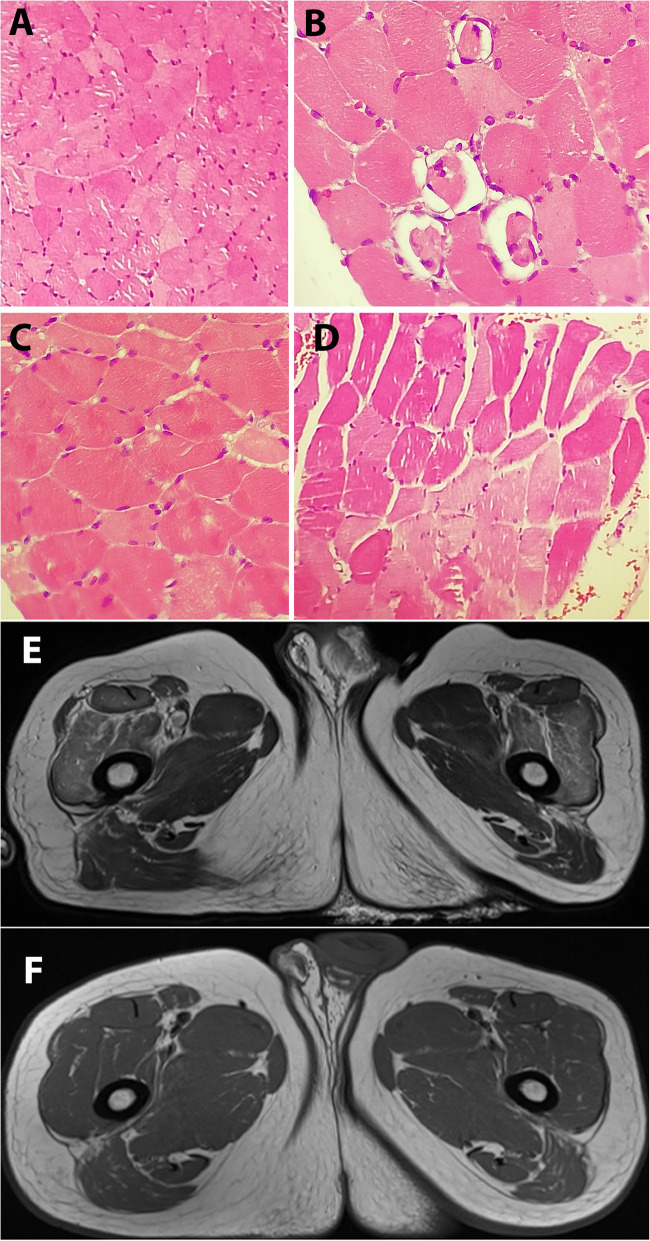
Case presentation: We addressed such a patient in his forties presented with features of severe SARS-CoV2 pneumonia and high serum CPK. He developed severe sepsis and acute respiratory distress syndrome (ARDS) and received intravenous high dose corticosteroid and tocilizumab to counter SARS-CoV2 associated cytokine surge. After 10 days of mechanical ventilation (MV), weaning was unsuccessful albeit apparently clear lung fields, having additionally severe and symmetric limb muscle weakness. Ancillary investigations in addition with serum CPK, including electromyogram, muscle biopsy, and muscle magnetic resonance imaging (MRI) suggested acute myopathy possibly due to skeletal myositis.
Conclusion: We wish to stress that myopathogenic medication in SARS-CoV2 pneumonia should be used with caution. Additionally, serum CPK could be a potential marker to predict respiratory failure in SARS-CoV2 pneumonia as skeletal myopathy affecting chest muscles may contribute ventilatory failure on top of oxygenation failure due to SARS-CoV2 pneumonia.
Keywords: Electromyogram; Guillain-Barré syndrome; Myopathy; Nerve conduction; SARS-CoV2.
Conflict of interest statement
No authors have financial, professional, or personal conflict of interest that may influence this manuscript to disclose.
Figures
References
-
- Tsai LK, Hsieh ST, Chao CCm, Chen YC, Lin YH, Chang SC, Chang YC Neuromuscular disorders in severe acute respiratory syndrome. Archives of neurology 2004; 61(11): 1669-1673, DOI: 10.1001/archneur.61.11.1669. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
