

The assessment of a manikin-based low-dose, high-frequency cardiac resuscitation quality improvement program in early UK adopter hospitals
- PMID: 33883025
- PMCID: PMC8058602
- DOI: 10.1186/s41077-021-00168-y
The assessment of a manikin-based low-dose, high-frequency cardiac resuscitation quality improvement program in early UK adopter hospitals
Abstract
Background: Adult and paediatric basic life support (BLS) training are often conducted via group training with an accredited instructor every 24 months. Multiple studies have demonstrated a decline in the quality of cardio-pulmonary resuscitation (CPR) performed as soon as 3-month post-training. The 'Resuscitation Quality Improvement' (RQI) programme is a quarterly low-dose, high-frequency training, based around the use of manikins connected to a cart providing real-time and summative feedback. We aimed to evaluate the effects of the RQI Programme on CPR psychomotor skills in UK hospitals that had adopted this as a method of BLS training, and establish whether this program leads to increased compliance in CPR training.
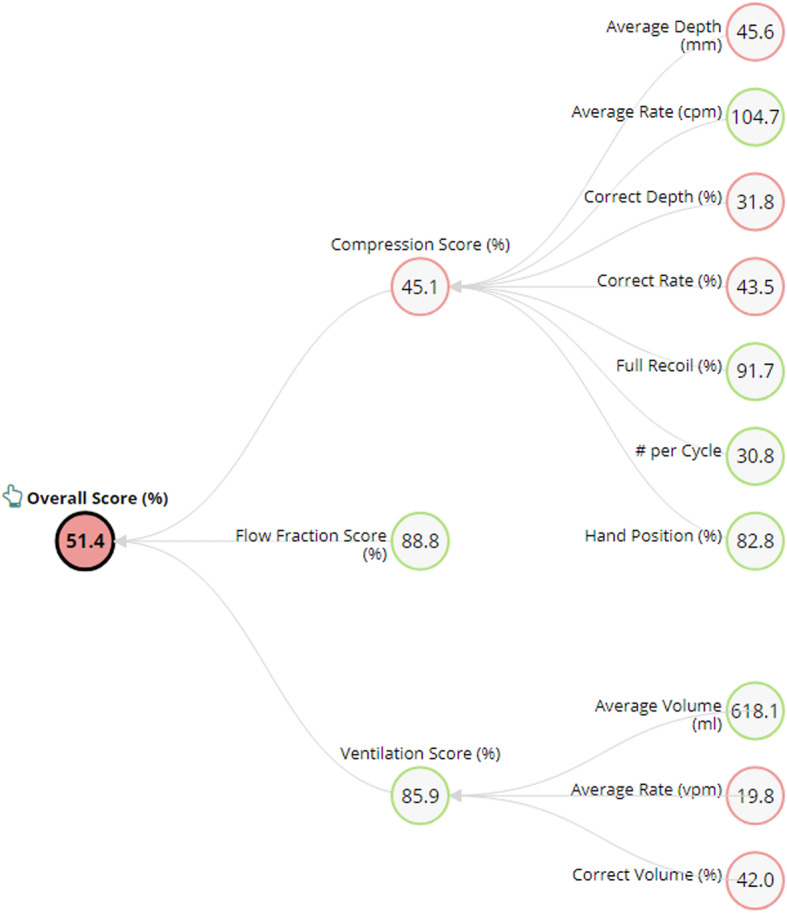
Methods: The study took place across three adopter sites and one control site. Participants completed a baseline assessment without live feedback. Following this, participants at the adopter sites followed the RQI curriculum for adult CPR, or adult and infant CPR. The curriculum was split into quarterly training blocks, and live feedback was given on technique during the training session via the RQI cart. After following the curriculum for 12/24 months, participants completed a second assessment without live feedback.
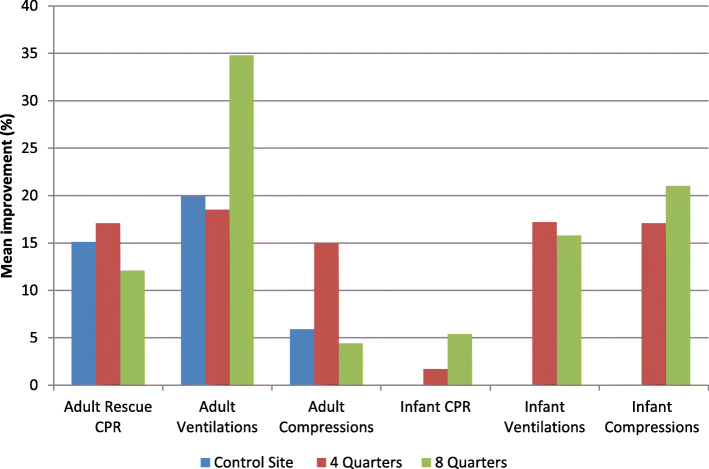
Results: At the adopter sites, there was a significant improvement in the overall score between baseline and assessment for infant ventilations (N = 167, p < 0.001), adult ventilations (n = 129, p < 0.001), infant compressions (n = 163, p < 0.001) adult compressions (n = 205, p < 0.001), and adult CPR (n = 249, p < 0.001). There was no significant improvement in the overall score for infant CPR (n = 206, p = 0.08). Data from the control site demonstrated a statistically significant improvement in mean score for adult CPR (n = 22, p = 0.02), but not for adult compressions (N = 18, p = 0.39) or ventilations (n = 17, p = 0.08). No statistically significant difference in improvement of mean scores was found between the grouped adopter sites and the control site. The effect of the duration of the RQI curriculum on CPR performance appeared to be minimal in this data set. Compliance with the RQI curriculum varied by site, one site maintained hospital compliance at 90% over a 1 year period, however compliance reduced over time at all sites.
Conclusions: This data demonstrated an increased adherence with guidelines for high-quality CPR post-training with the RQI cart, for all adult and most infant measures, but not infant CPR. However, the relationship between a formalised quarterly RQI curriculum and improvements in resuscitation skills is not clear. It is also unclear whether the RQI approach is superior to the current classroom-based BLS training for CPR skill acquisition in the UK. Further research is required to establish how to optimally implement the RQI system in the UK and how to optimally improve hospital wide compliance with CPR training to improve the outcomes of in-hospital cardiac arrests.
Keywords: Cardiopulmonary resuscitation; Simulation; Training.
Conflict of interest statement
This work was in part funded Laerdal Medical. These funds covered the salary of study staff for time spent working on the study. NH is substantively employed by the British Heart Foundation.
Figures





References
-
- Meaney PA, Bobrow BJ, Mancini ME, Christenson J, de Caen AR, Bhanji F, et al. Cardiopulmonary resuscitation quality: [corrected] improving cardiac resuscitation outcomes both inside and outside the hospital: a consensus statement from the American Heart Association. Circulation. 2013;128(4):417–435. doi: 10.1161/CIR.0b013e31829d8654. - DOI - PubMed
-
- Audit NCA . Key statistics from the National Cardiac Arrest Audit 2018/19. 2019.
-
- Sutton RM, Wolfe H, Nishisaki A, Leffelman J, Niles D, Meaney PA, et al. Pushing harder, pushing faster, minimizing interruptions… but falling short of 2010 cardiopulmonary resuscitation targets during in-hospital pediatric and adolescent resuscitation. Resuscitation. 2013;84(12):1680–1684. doi: 10.1016/j.resuscitation.2013.07.029. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
