

Contribution of Racial and Ethnic Differences in Cerebral Small Vessel Disease Subtype and Burden to Risk of Cerebral Hemorrhage Recurrence
- PMID: 33883240
- PMCID: PMC8205476
- DOI: 10.1212/WNL.0000000000011932
Contribution of Racial and Ethnic Differences in Cerebral Small Vessel Disease Subtype and Burden to Risk of Cerebral Hemorrhage Recurrence
Abstract
Objective: Black and Hispanic survivors of intracerebral hemorrhage (ICH) are at higher risk of recurrent intracranial bleeding. MRI-based markers of chronic cerebral small vessel disease (CSVD) are consistently associated with recurrent ICH. We therefore sought to investigate whether racial/ethnic differences in MRI-defined CSVD subtype and severity contribute to disparities in ICH recurrence risk.
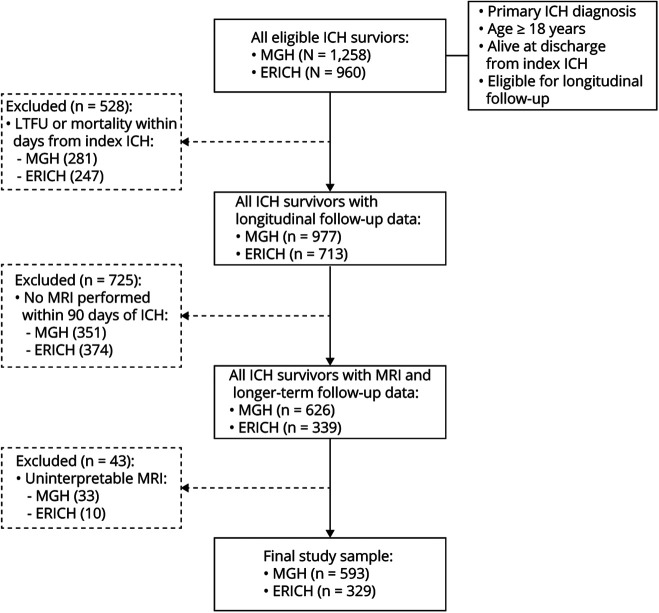
Methods: We analyzed data from the Massachusetts General Hospital ICH study (n = 593) and the Ethnic/Racial Variations of Intracerebral Hemorrhage (ERICH) study (n = 329). Using CSVD markers derived from MRIs obtained within 90 days of index ICH, we classified ICH cases as cerebral amyloid angiopathy (CAA)-related, hypertensive arteriopathy (HTNA)-related, and mixed etiology. We quantified CSVD burden using validated global, CAA-specific, and HTNA-specific scores. We compared CSVD subtype and severity among White, Black, and Hispanic ICH survivors and investigated its association with ICH recurrence risk.
Results: We analyzed data for 922 ICH survivors (655 White, 130 Black, 137 Hispanic). Minority ICH survivors had greater global CSVD (p = 0.011) and HTNA burden (p = 0.021) on MRI. Furthermore, minority survivors of HTNA-related and mixed-etiology ICH demonstrated higher HTNA burden, resulting in increased ICH recurrence risk (all p < 0.05).
Conclusions: We uncovered significant differences in CSVD subtypes and severity among White and minority survivors of primary ICH, with direct implication for known disparities in ICH recurrence risk. Future studies of racial/ethnic disparities in ICH outcomes will benefit from including detailed MRI-based assessment of CSVD subtypes and severity and investigating social determinants of health.
© 2021 American Academy of Neurology.
Figures


References
-
- Poon MT, Fonville AF, Al-Shahi Salman R. Long-term prognosis after intracerebral haemorrhage: systematic review and meta-analysis. J Neurol Neurosurg Psychiatry. 2014;85(6):660-667. - PubMed
-
- Gonzalez-Perez A, Gaist D, Wallander MA, McFeat G, Garcia-Rodriguez LA. Mortality after hemorrhagic stroke: data from general practice (The Health Improvement Network). Neurology. 2013;81(6):559-565. - PubMed
-
- Bae H, Jeong D, Doh J, Lee K, Yun I, Byun B. Recurrence of bleeding in patients with hypertensive intracerebral hemorrhage. Cerebrovasc Dis. 1999;9(2):102-108. - PubMed
-
- Bailey RD, Hart RG, Benavente O, Pearce LA. Recurrent brain hemorrhage is more frequent than ischemic stroke after intracranial hemorrhage. Neurology. 2001;56(6):773-777. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources