

Exploring the Complexity of Death-Censored Kidney Allograft Failure
- PMID: 33883251
- PMCID: PMC8259637
- DOI: 10.1681/ASN.2020081215
Exploring the Complexity of Death-Censored Kidney Allograft Failure
Abstract
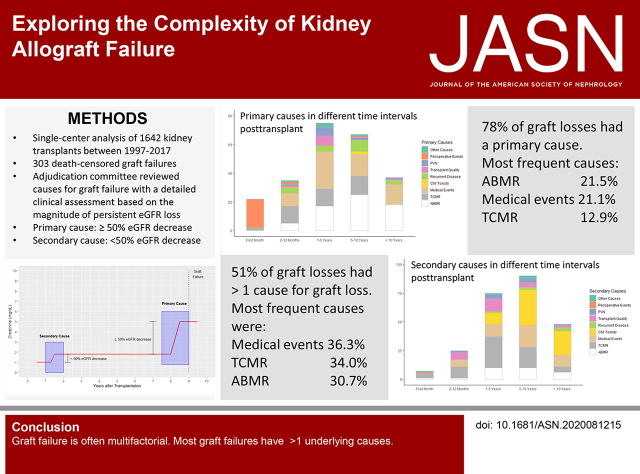
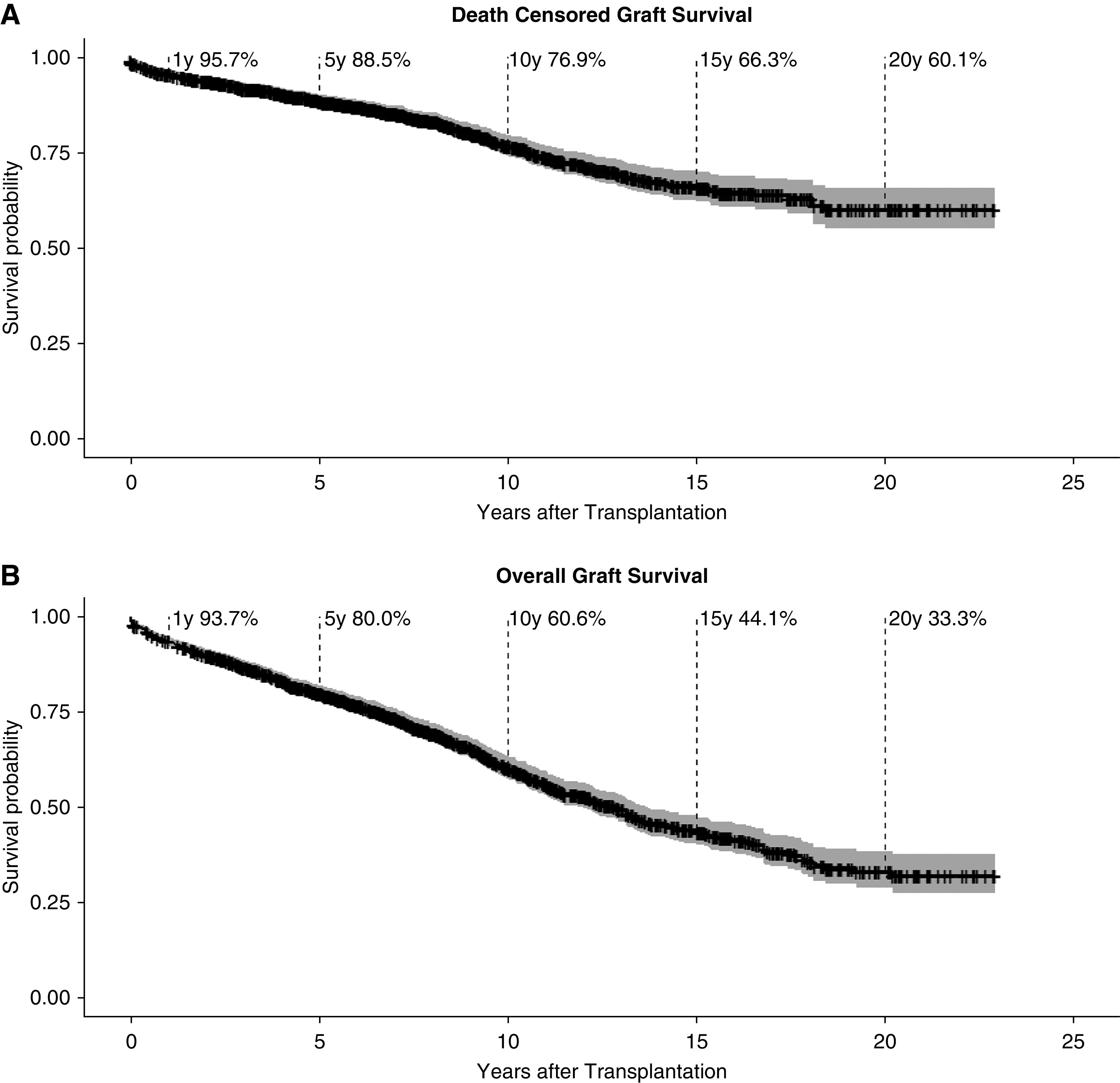
Background: Few studies have thoroughly investigated the causes of kidney graft loss (GL), despite its importance.
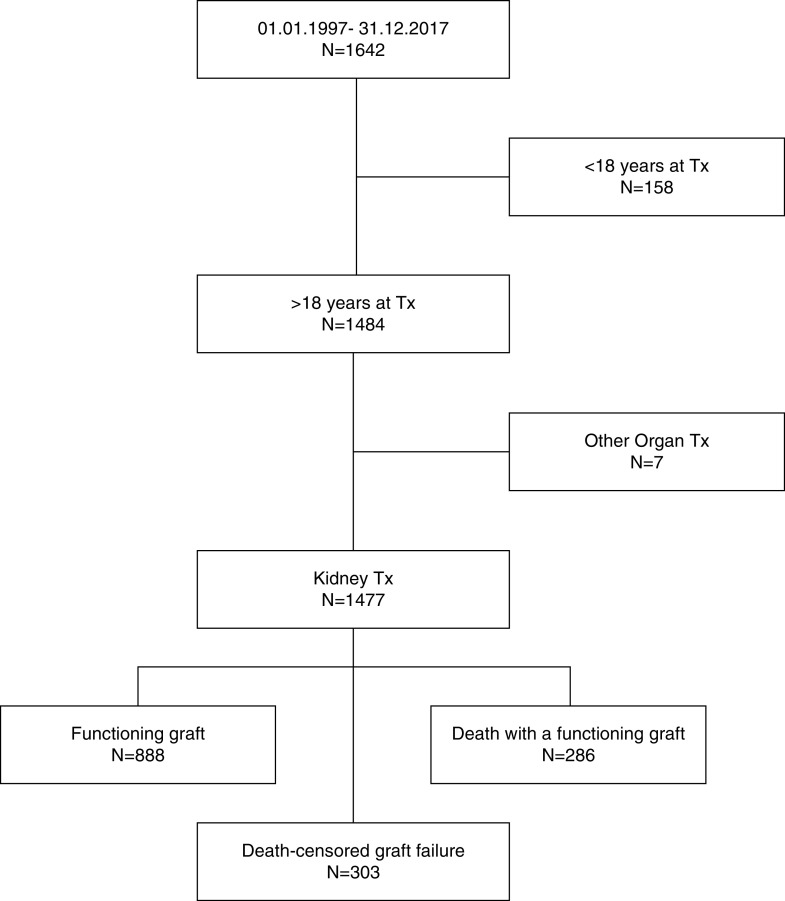
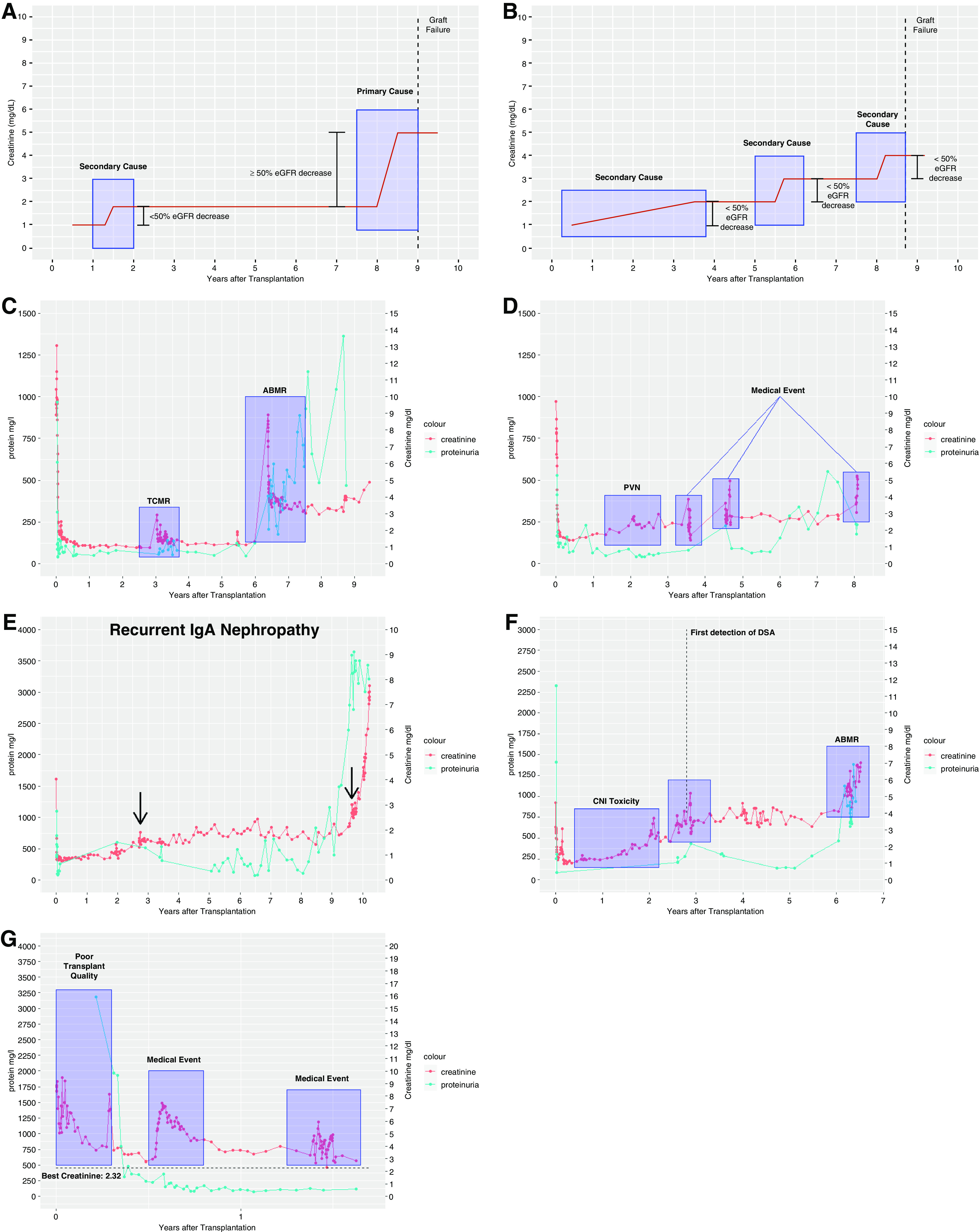
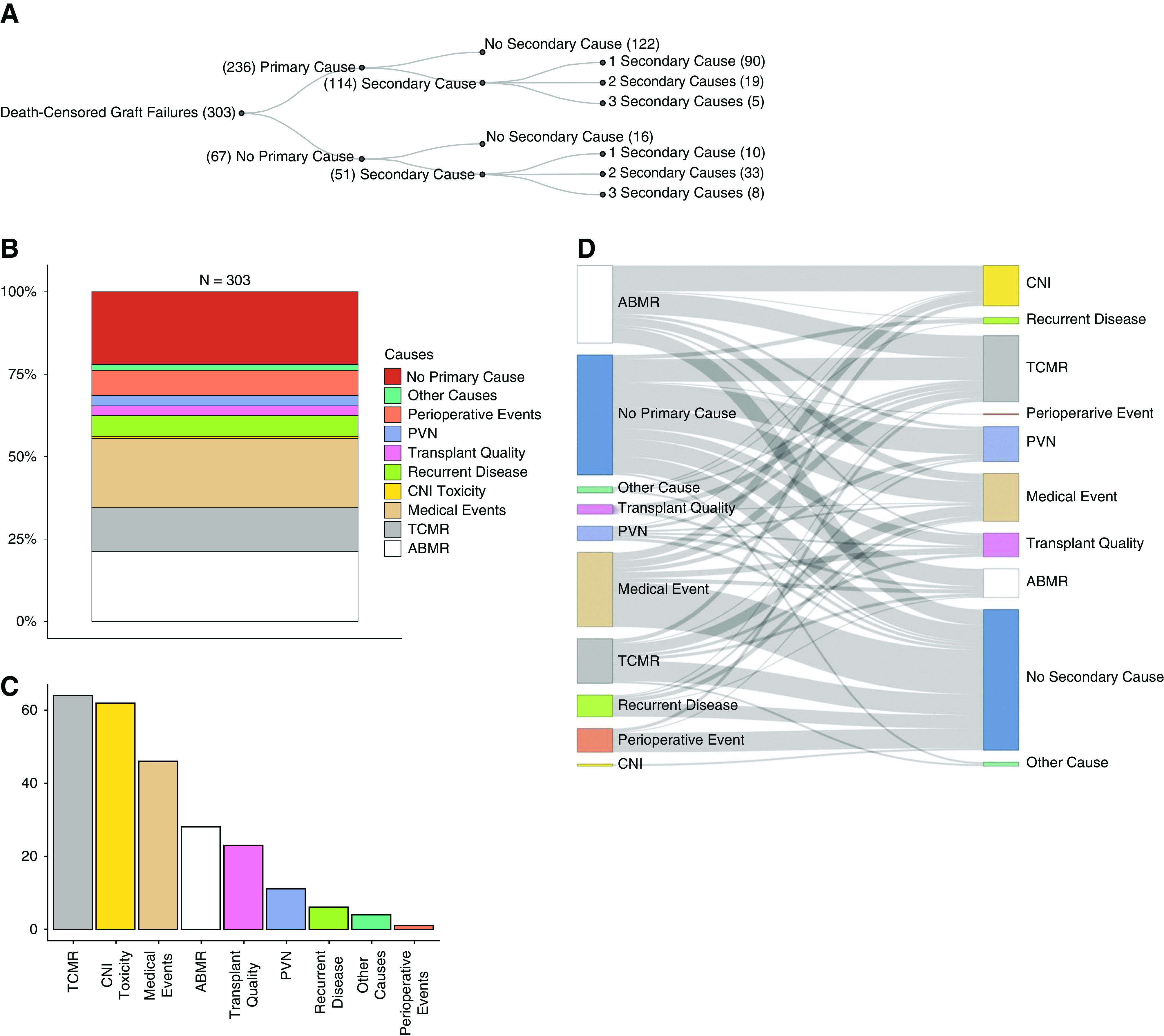
Methods: A novel approach assigns each persistent and relevant decline in renal function over the lifetime of a renal allograft to a standardized category, hypothesizing that singular or multiple events finally lead to GL. An adjudication committee of three physicians retrospectively evaluated indication biopsies, laboratory testing, and medical history of all 303 GLs among all 1642 recipients of transplants between January 1, 1997 and December 31, 2017 at a large university hospital to assign primary and/or secondary causes of GL.
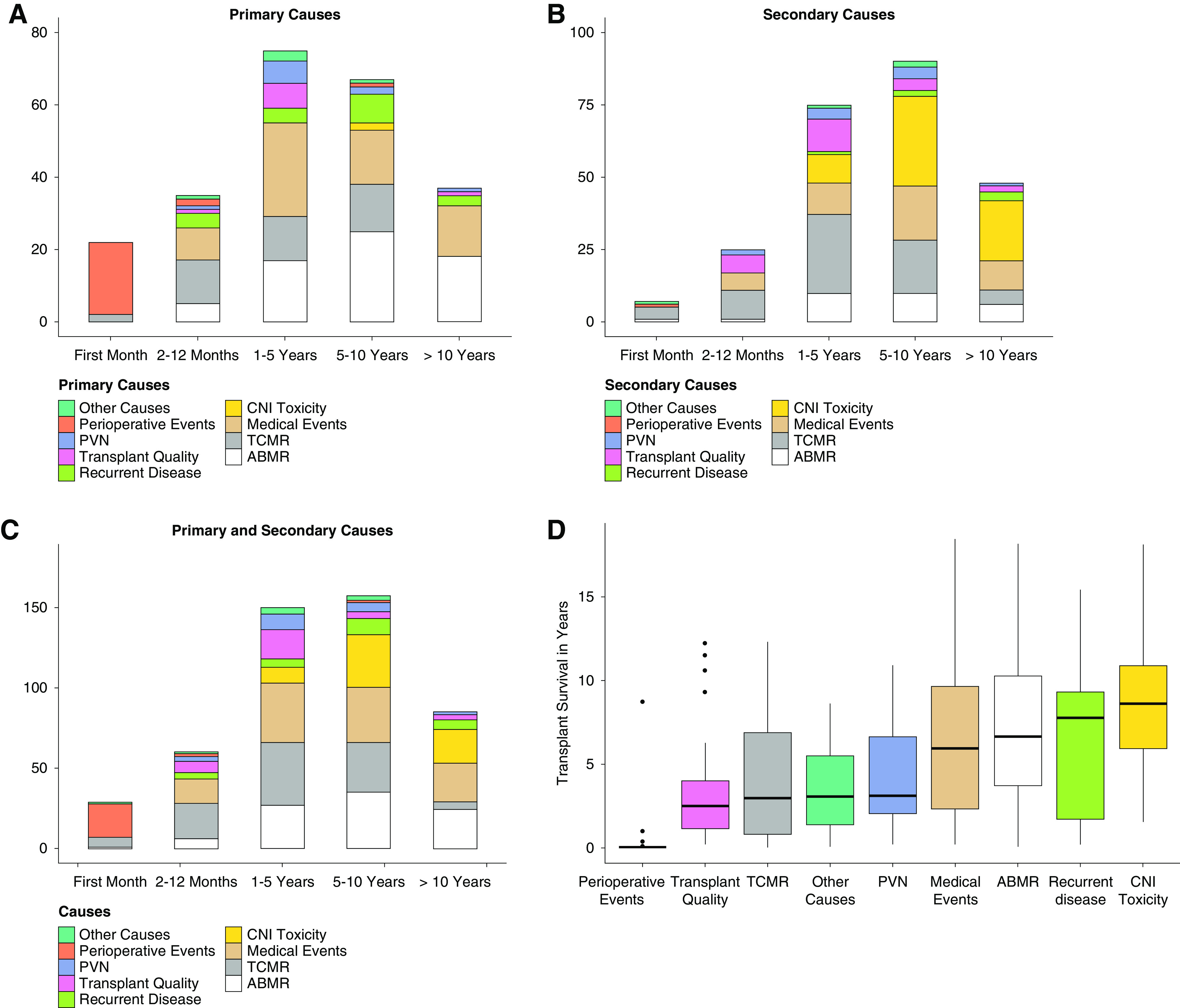
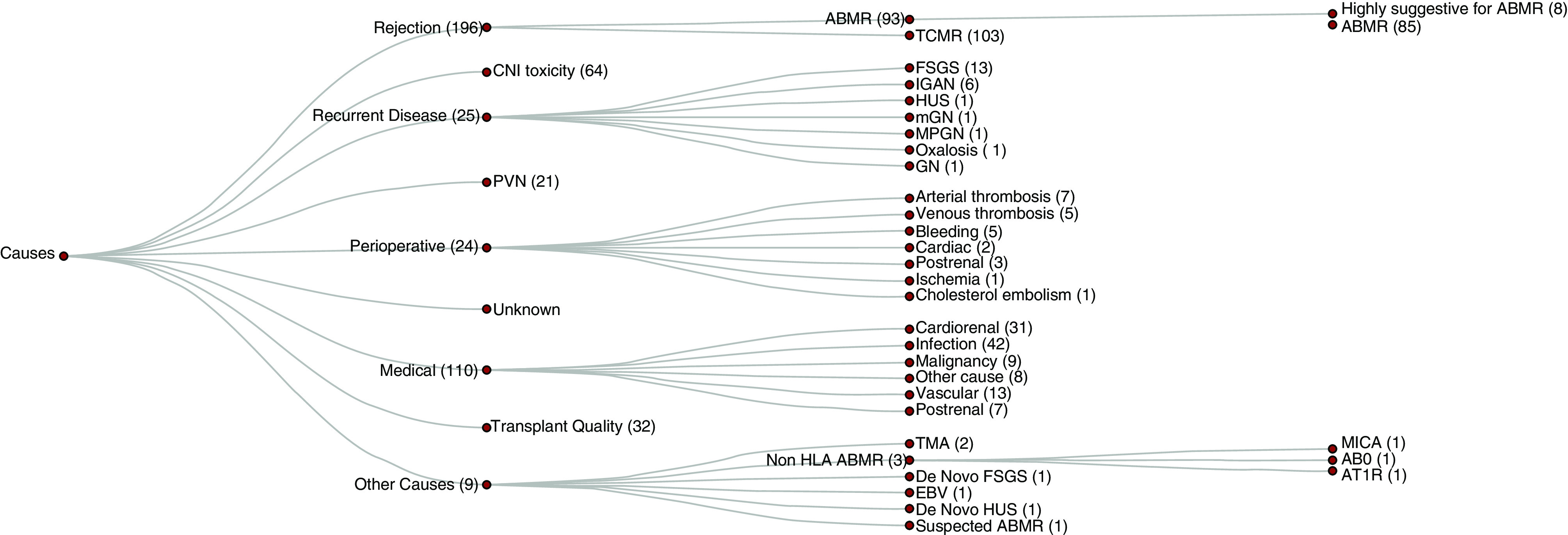
Results: In 51.2% of the patients, more than one cause contributed to GL. The most frequent primary or secondary causes leading to graft failure were intercurrent medical events in 36.3% of graft failures followed by T cell-mediated rejection (TCMR) in 34% and antibody-mediated rejection (ABMR) in 30.7%. In 77.9%, a primary cause could be attributed to GL, of which ABMR was most frequent (21.5%). Many causes for GL were identified, and predominant causes for GL varied over time.
Conclusions: GL is often multifactorial and more complex than previously thought.
Keywords: chronic allograft failure; clinical nephrology; transplant outcomes; transplant pathology; transplantation.
Copyright © 2021 by the American Society of Nephrology.
Figures
References
-
- Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, et al. .: Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med 341: 1725–1730, 1999. - PubMed
-
- Suthanthiran M, Strom TB: Renal transplantation. N Engl J Med 331: 365–376, 1994. - PubMed
-
- Schnuelle P, Lorenz D, Trede M, Van Der Woude FJ: Impact of renal cadaveric transplantation on survival in end-stage renal failure: Evidence for reduced mortality risk compared with hemodialysis during long-term follow-up. J Am Soc Nephrol 9: 2135–2141, 1998. - PubMed
-
- Oniscu GC, Brown H, Forsythe JL: Impact of cadaveric renal transplantation on survival in patients listed for transplantation. J Am Soc Nephrol 16: 1859–1865, 2005. - PubMed
-
- Valderrábano F, Jofre R, López-Gómez JM: Quality of life in end-stage renal disease patients. Am J Kidney Dis 38: 443–464, 2001. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
