

Prediction of sarcopenia using a battery of circulating biomarkers
- PMID: 33883602
- PMCID: PMC8060253
- DOI: 10.1038/s41598-021-87974-6
Prediction of sarcopenia using a battery of circulating biomarkers
Abstract
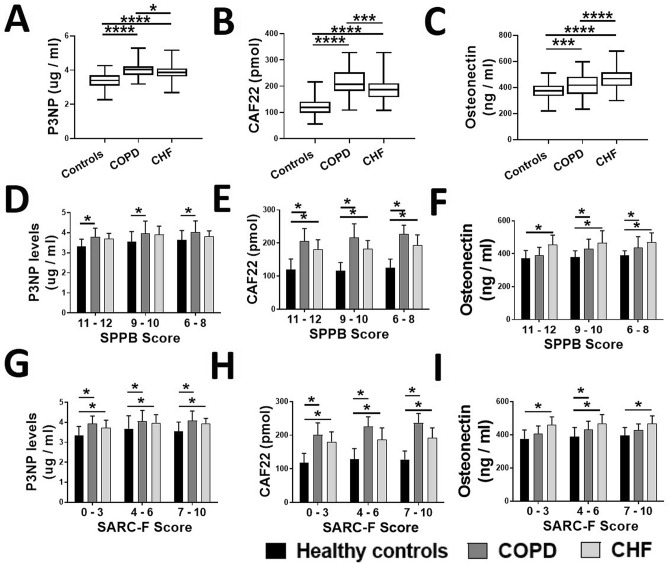
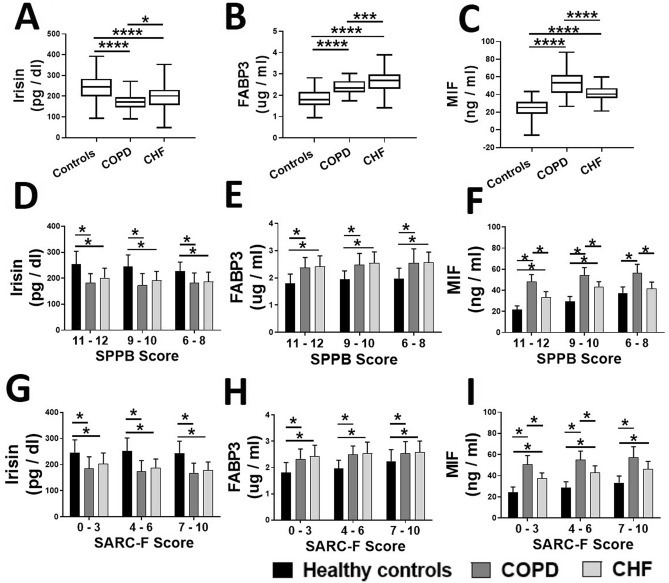
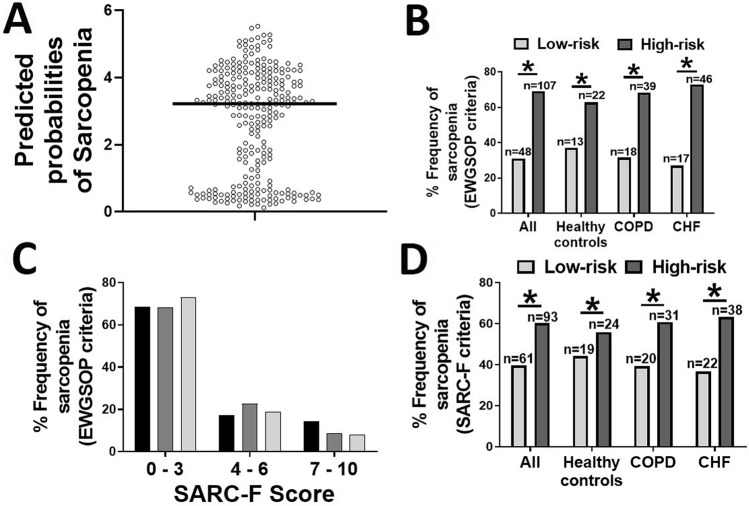
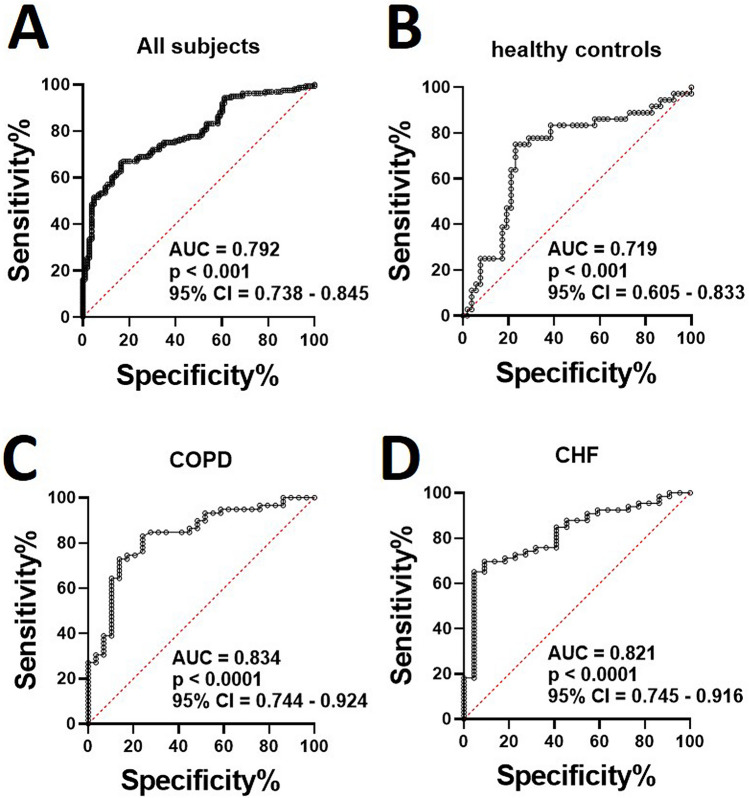
Loss of muscle mass and strength with aging, termed sarcopenia is accelerated in several comorbidities including chronic heart failure (CHF) and chronic obstructive pulmonary diseases (COPD). However, the effective circulating biomarkers to accurately diagnose and assess sarcopenia are not known. We recruited male healthy controls and patients with CHF and COPD (n = 81-87/group), aged 55-74 years. Sarcopenia was clinically identified based on hand-grip strength, appendicular skeletal muscle index and physical capacity as recommended by the European working group for sarcopenia. The serum levels of amino-terminal pro-peptide of type-III procollagen, c-terminal agrin fragment-22, osteonectin, irisin, fatty acid-binding protein-3 and macrophage migration inhibitory factor were significantly different between healthy controls and patients with CHF and COPD. Risk scores for individual biomarkers were calculated by logistic regressions and combined into a cumulative risk score. The median cutoff value of 3.86 was used to divide subjects into high- and low-risk groups for sarcopenia with the area under the curve of 0.793 (95% CI = 0.738-0.845, p < 0.001). A significantly higher incidence of clinical sarcopenia was found in high-risk group. Taken together, the battery of biomarkers can be an effective tool in the early diagnosis and assessment of sarcopenia.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
