

Sequential Organ Failure Assessment Score As a Predictor of Outcome in Sepsis in Pediatric Intensive Care Unit
- PMID: 33884211
- PMCID: PMC8052111
- DOI: 10.1055/s-0040-1714705
Sequential Organ Failure Assessment Score As a Predictor of Outcome in Sepsis in Pediatric Intensive Care Unit
Abstract
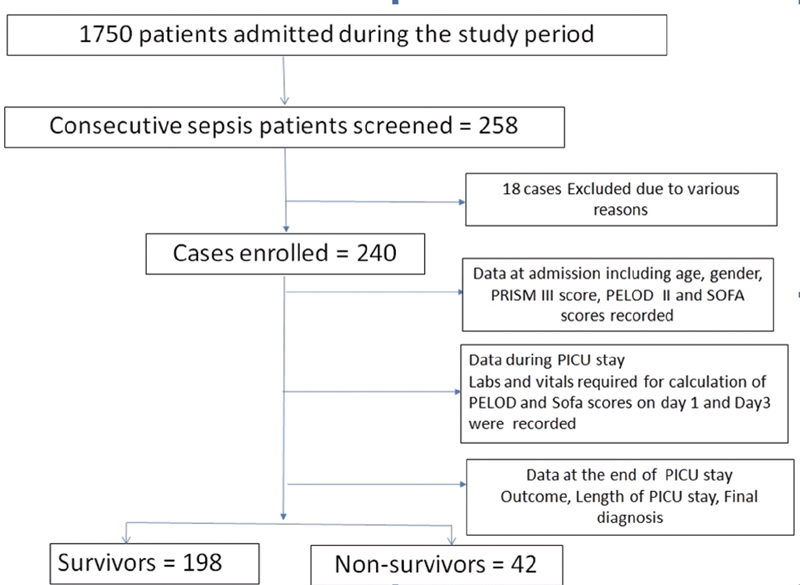
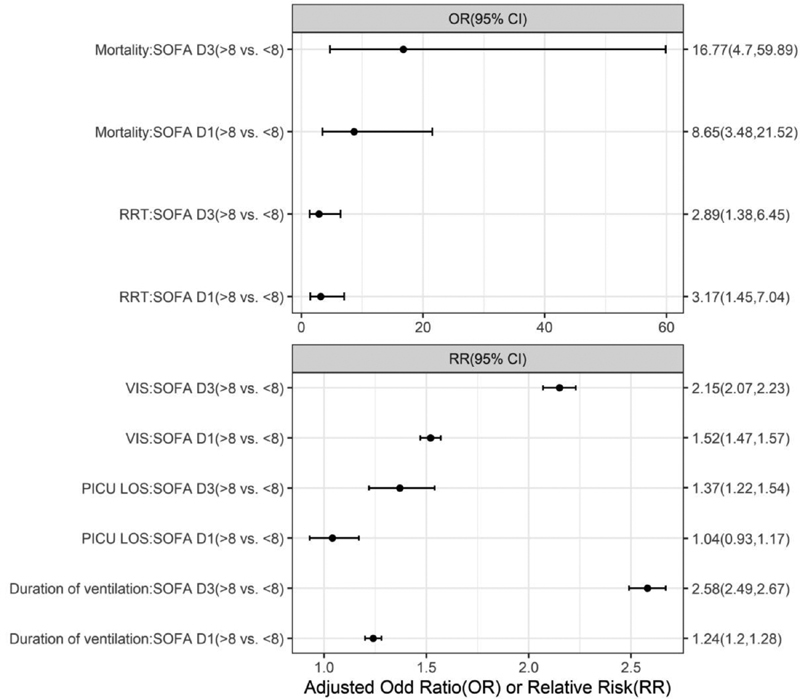
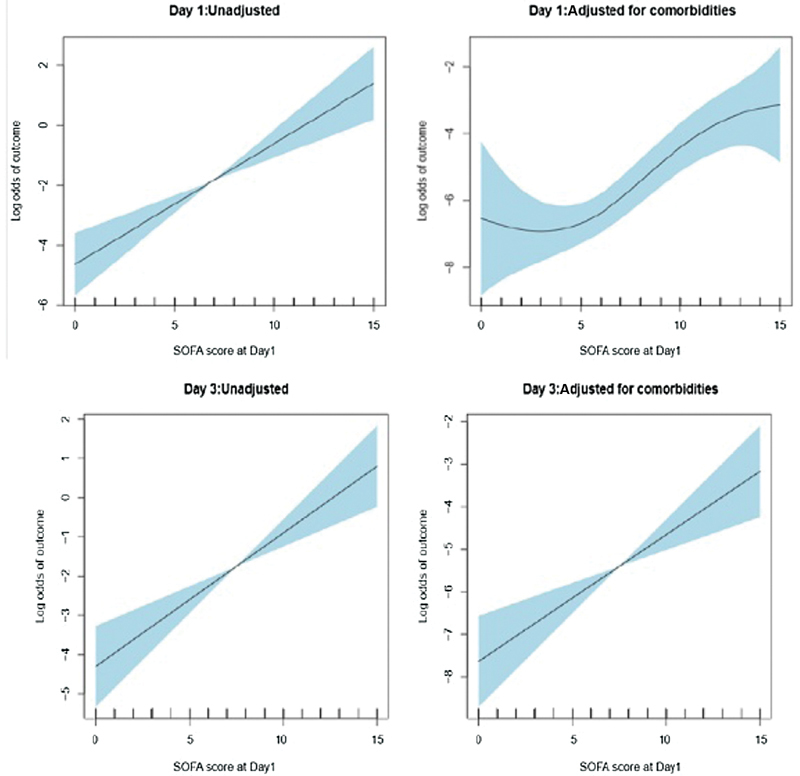
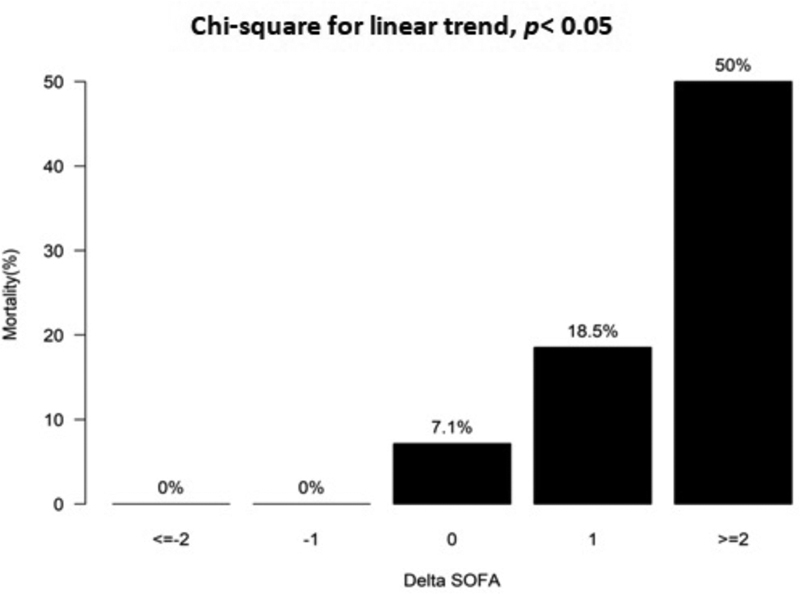
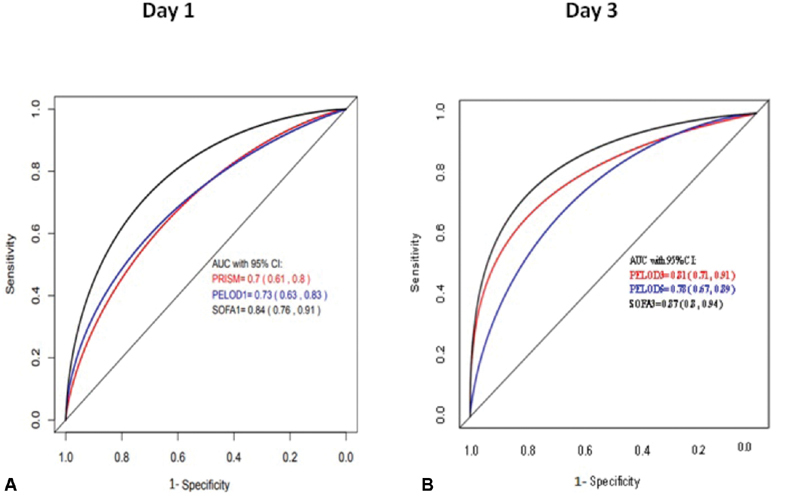
Sequential organ failure assessment (SOFA) score is used as a predictor of outcome of sepsis in the pediatric intensive care unit. The aim of the study is to determine the application of SOFA scores as a predictor of outcome in children admitted to the pediatric intensive care unit with a diagnosis of sepsis. The design involved is prospective observational study. The study took place at the multidisciplinary pediatric intensive care unit (PICU), tertiary care hospital, South India. The patients included are children, aged 1 month to 18 years admitted with a diagnosis of sepsis (suspected/proven) to a single center PICU in India from November 2017 to November 2019. Data collected included the demographic, clinical, laboratory, and outcome-related variables. Severity of illness scores was calculated to include SOFA score day 1 (SF1) and day 3 (SF3) using a pediatric version (pediatric SOFA score or pSOFA) with age-adjusted cutoff variables for organ dysfunction, pediatric risk of mortality III (PRISM III; within 24 hours of admission), and pediatric logistic organ dysfunction-2 or PELOD-2 (days 1, 3, and 5). A total of 240 patients were admitted to the PICU with septic shock during the study period. The overall mortality rate was 42 of 240 patients (17.5%). The majority (59%) required mechanical ventilation, while only 19% required renal replacement therapy. The PRISM III, PELOD-2, and pSOFA scores correlated well with mortality. All three severity of illness scores were higher among nonsurvivors as compared with survivors ( p < 0.001). pSOFA scores on both day 1 (area under the curve or AUC 0.84) and day 3 (AUC 0.87) demonstrated significantly higher discriminative power for in-hospital mortality as compared with PRISM III (AUC, 0.7), and PELOD-2 (day 1, [AUC, 0.73]), and PELOD-2 (day 3, [AUC, 0.81]). Utilizing a cutoff SOFA score of >8, the relative risk of prolonged duration of mechanical ventilation, requirement for vasoactive infusions (vasoactive infusion score), and PICU length of stay were all significantly increased ( p < 0.05), on both days 1 and 3. On multiple logistic regression, adjusted odds ratio of mortality was elevated at 8.65 (95% CI: 3.48-21.52) on day 1 and 16.77 (95% confidence interval or CI: 4.7-59.89) on day 3 ( p < 0.001) utilizing the same SOFA score cutoff of 8. A positive association was found between the delta SOFA ([Δ] SOFA) from day 1 to day 3 (SF1-SF3) and in-hospital mortality (chi-square for linear trend, p < 0.001). Subjects with a ΔSOFA of ≥2 points had an exponential mortality rate to 50%. Similar association was-observed between ΔSOFA of ≥2 and-longer duration of inotropic support ( p = 0.0006) with correlation co-efficient 0.2 (95% CI: 0.15-0.35; p = 0.01). Among children admitted to the PICU with septic shock, SOFA scores on both days 1 and 3, have a greater discriminative power for predicting in-hospital mortality than either PRISM III score (within 24 hours of admission) or PELOD-2 score (days 1 and 3). An increase in ΔSOFA of >2 adds additional prognostic accuracy in determining not only mortality risk but also duration of inotropic support as well.
Keywords: PELOD-2; PRISM III; SOFA score; outcome prediction; septic shock.
Thieme. All rights reserved.
Conflict of interest statement
Conflict of Interest None declared.
Figures
Similar articles
-
The Various Scoring Systems in Pediatric Intensive Care Units: A Prospective Observational Study.Cureus. 2023 May 30;15(5):e39679. doi: 10.7759/cureus.39679. eCollection 2023 May. Cureus. 2023. PMID: 37398718 Free PMC article.
-
Adaptation and Validation of a Pediatric Sequential Organ Failure Assessment Score and Evaluation of the Sepsis-3 Definitions in Critically Ill Children.JAMA Pediatr. 2017 Oct 2;171(10):e172352. doi: 10.1001/jamapediatrics.2017.2352. Epub 2017 Oct 2. JAMA Pediatr. 2017. PMID: 28783810 Free PMC article.
-
[Paediatric sequential organ failure assessment (pSOFA) score: A new mortality prediction score in the paediatric intensive care unit].An Pediatr (Engl Ed). 2020 May;92(5):277-285. doi: 10.1016/j.anpedi.2019.05.018. Epub 2019 Nov 26. An Pediatr (Engl Ed). 2020. PMID: 31784324 Spanish.
-
[Meta analysis of the predictive efficacy of various derived indicators of sequential organ failure assessment in outcomes of patients with sepsis].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024 Mar;36(3):249-255. doi: 10.3760/cma.j.cn121430-20231007-00843. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024. PMID: 38538352 Chinese.
-
Pediatric Sequential Organ Assessment Score: A Comprehensive Review of the Prognostic Marker in the Pediatric Intensive Care Unit.Cureus. 2024 May 10;16(5):e60034. doi: 10.7759/cureus.60034. eCollection 2024 May. Cureus. 2024. PMID: 38854197 Free PMC article. Review.
Cited by
-
Epidemiology of pediatric sepsis in the pediatric intensive care unit of king Abdulaziz Medical City, Jeddah, Saudi Arabia.BMC Pediatr. 2021 May 7;21(1):222. doi: 10.1186/s12887-021-02686-0. BMC Pediatr. 2021. PMID: 33962589 Free PMC article.
-
Comparison between hospital- and community-acquired septic shock in children: a single-center retrospective cohort study.World J Pediatr. 2022 Nov;18(11):734-745. doi: 10.1007/s12519-022-00574-w. Epub 2022 Jun 23. World J Pediatr. 2022. PMID: 35737181 Free PMC article.
-
Serum amyloid A and proadrenomedullin as early markers in critically ill children with sepsis.Clin Exp Pediatr. 2025 Aug;68(8):578-586. doi: 10.3345/cep.2024.01928. Epub 2025 Feb 26. Clin Exp Pediatr. 2025. PMID: 40017271 Free PMC article.
-
Neonatal Sequential Organ Failure Assessment as a late-onset sepsis mortality predictor in very low birth weight newborns: a Brazilian cohort study.Eur J Pediatr. 2022 Oct;181(10):3767-3774. doi: 10.1007/s00431-022-04583-9. Epub 2022 Aug 18. Eur J Pediatr. 2022. PMID: 35982172
-
The Various Scoring Systems in Pediatric Intensive Care Units: A Prospective Observational Study.Cureus. 2023 May 30;15(5):e39679. doi: 10.7759/cureus.39679. eCollection 2023 May. Cureus. 2023. PMID: 37398718 Free PMC article.
References
-
- Fisher J D, Nelson D G, Beyersdorf H, Satkowiak L J. Clinical spectrum of shock in the pediatric emergency department. Pediatr Emerg Care. 2010;26(09):622–625. - PubMed
-
- Shanley T P, Hallstrom C, Wong H R.Pediatric Critical Care—4th EditionAccessed November 3, 2019 at:https://www.elsevier.com/books/pediatric-critical-care/Fuhrman/978-0-323...
-
- American College of Critical Care Medicine Task Force Committee Members . Carcillo J A, Fields A I. Clinical practice parameters for hemodynamic support of pediatric and neonatal patients in septic shock. Crit Care Med. 2002;30(06):1365–1378. - PubMed
-
- Sarthi M, Lodha R, Vivekanandhan S, Arora N K. Adrenal status in children with septic shock using low-dose stimulation test. Pediatr Crit Care Med. 2007;8(01):23–28. - PubMed
-
- Beal A L, Cerra F B. Multiple organ failure syndrome in the 1990s. Systemic inflammatory response and organ dysfunction. JAMA. 1994;271(03):226–233. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
