

doi: 10.1016/j.vgie.2020.10.004.
eCollection 2021 Feb.
Endoscopic submucosal dissection for superficial pharyngeal carcinoma using transnasal endoscope
Affiliations
- PMID: 33884330
- PMCID: PMC7859500
- DOI: 10.1016/j.vgie.2020.10.004
Item in Clipboard
Endoscopic submucosal dissection for superficial pharyngeal carcinoma using transnasal endoscope
VideoGIE.
.
No abstract available
Keywords: ESD, endoscopic submucosal dissection.
Figures
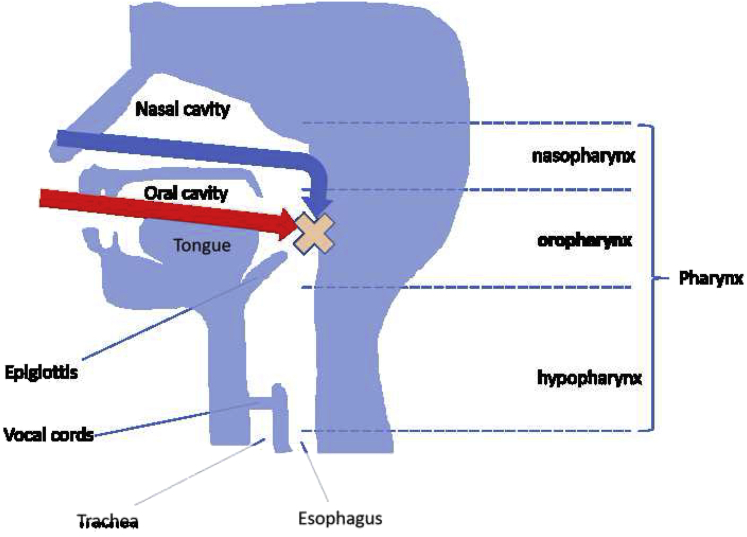
Schema of the pharynx. The posterior wall of the oropharynx is seen vertically via the transoral endoscope (red arrow). With the transnasal endoscope, the lesion can be approached horizontally (blue arrow).
Endoscopic image of marking. A 25-mm area unstained with iodine is seen on the right side of the posterior oropharyngeal wall.
Endoscopic image during mucosal incision (transoral endoscope). Circumferential incision performed via conventional endoscopy.
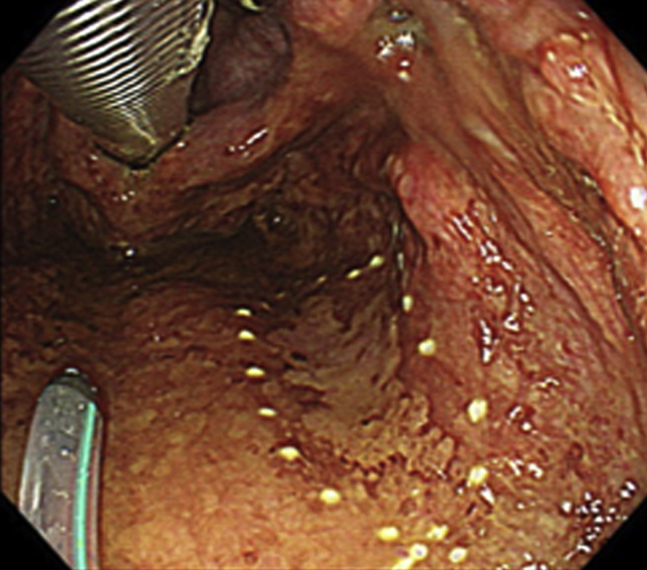
Endoscopic image during dissection (transoral endoscope). Entry into the subepithelial layer circumferential incision is difficult because the subepithelial tissue is thin and perpendicular to the muscle layer.
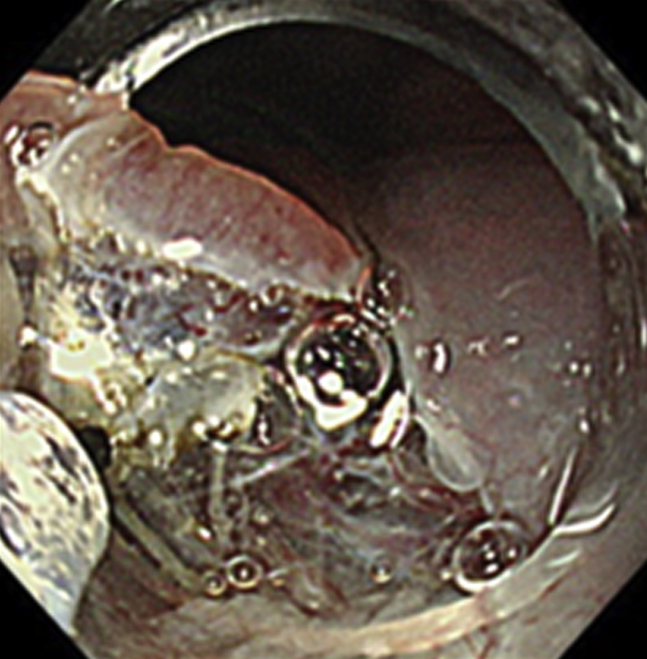
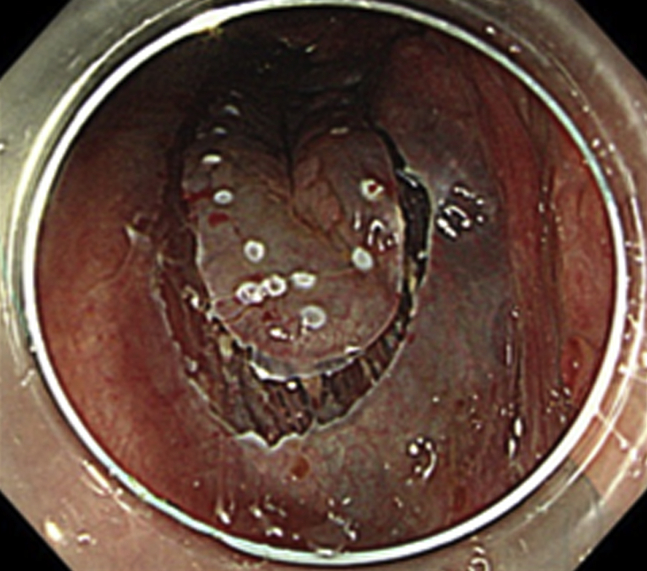
Endoscopic image during dissection (transnasal endoscope). Horizontal approach to the lesion is possible. Entry into the narrow subepithelial space is easy because of the thin endoscope.
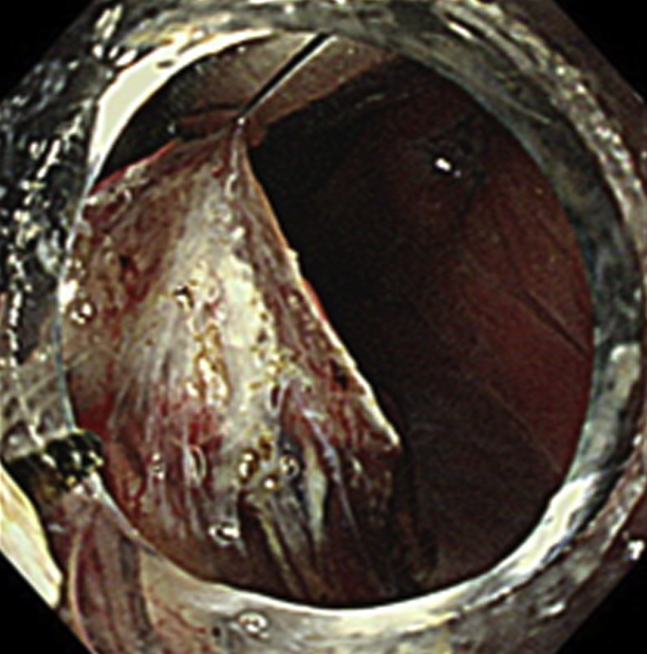
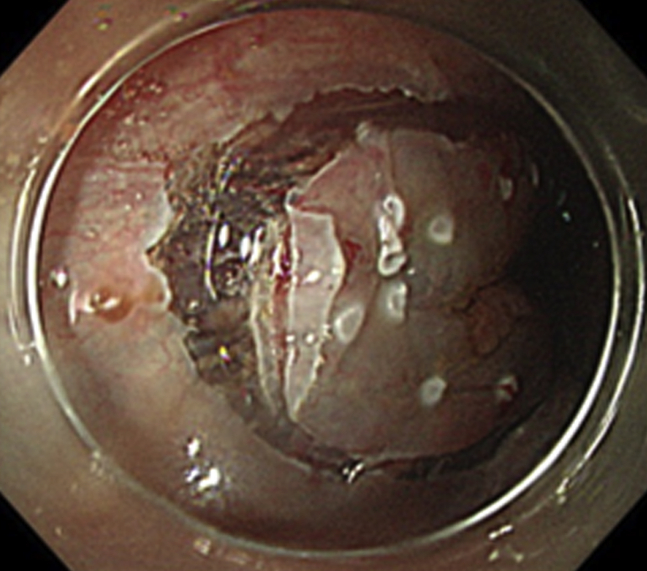
Endoscopic image during dissection (transnasal endoscope). Subepithelial tissue could be dissected under direct vision. Laryngeal forceps inserted orally are useful for applying traction.
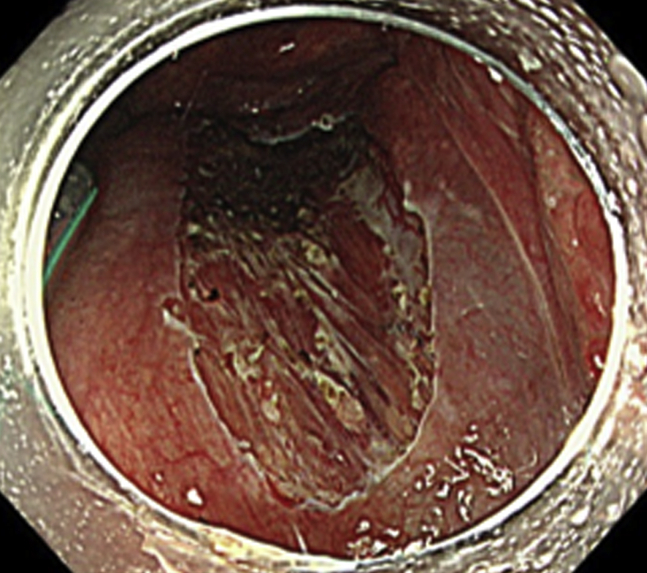
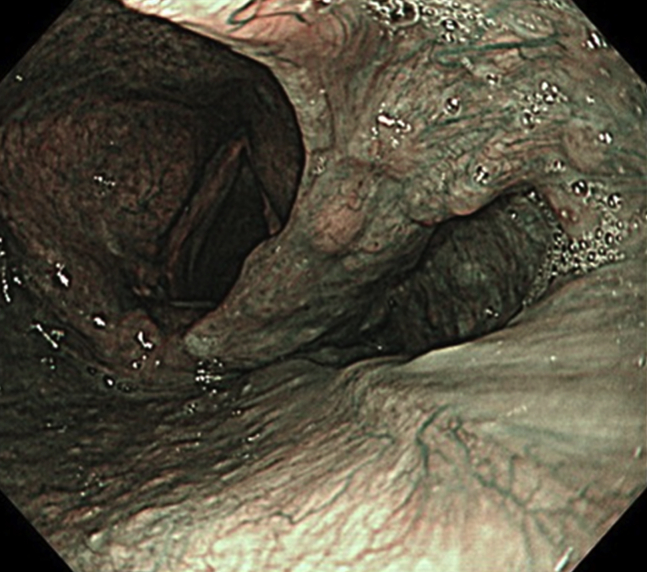
Endoscopic submucosal dissection ulcer after resection. The lesion was resected en bloc without adverse events.
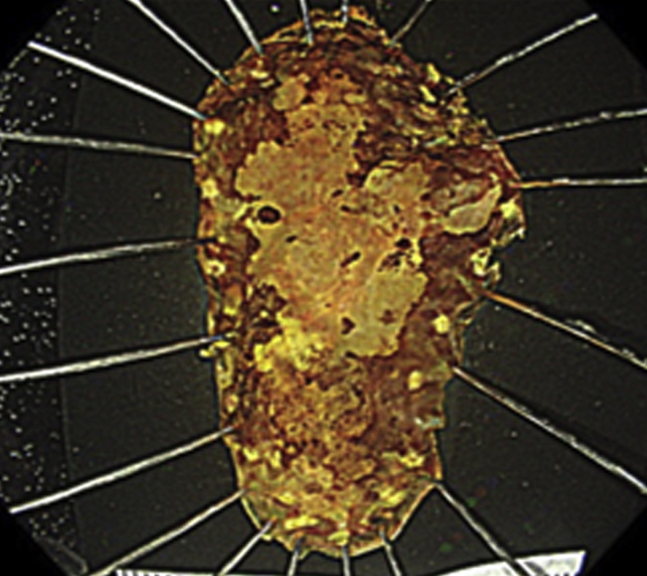
Endoscopic submucosal dissection specimen. The lesion was squamous cell carcinoma in situ, measuring 25×14 mm, ly0, v0, margin negative.
Two months after endoscopic submucosal dissection. Endoscopic submucosal dissection ulcer was completely healed.
References
-
- Kikuchi D., Iizuka T., Yamada A. Utility of magnifying endoscopy with narrow band imaging in determining the invasion depth of superficial pharyngeal cancer. Head Neck. 2015;37:846–850. - PubMed
-
- Hanaoka N., Ishihara R., Takeuchi Y. Endoscopic submucosal dissection as minimally invasive treatment for superficial pharyngeal cancer: a phase II study (with video) Gastrointest Endosc. 2015;82:1002–1008. - PubMed
-
- Iizuka T., Kikuchi D., Hoteya S. Endoscopic submucosal dissection for treatment of mesopharyngeal and hypopharyngeal carcinomas. Endoscopy. 2009;41:113–117. - PubMed
-
- Iizuka T., Kikuchi D., Hoteya S. A new technique for pharyngeal endoscopic submucosal dissection: peroral countertraction (with video) Gastrointest Endosc. 2012;76:1034–1038. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
