

Gender differences in the provision of intensive care: a Bayesian approach
- PMID: 33884452
- PMCID: PMC8139895
- DOI: 10.1007/s00134-021-06393-3
Gender differences in the provision of intensive care: a Bayesian approach
Abstract
Purpose: It is currently unclear whether management and outcomes of critically ill patients differ between men and women. We sought to assess the influence of age, sex and diagnoses on the probability of intensive care provision in critically ill cardio- and neurovascular patients in a large nationwide cohort in Switzerland.
Methods: Retrospective analysis of 450,948 adult patients with neuro- and cardiovascular disease admitted to all hospitals in Switzerland between 01/2012 and 12/2016 using Bayesian modeling.
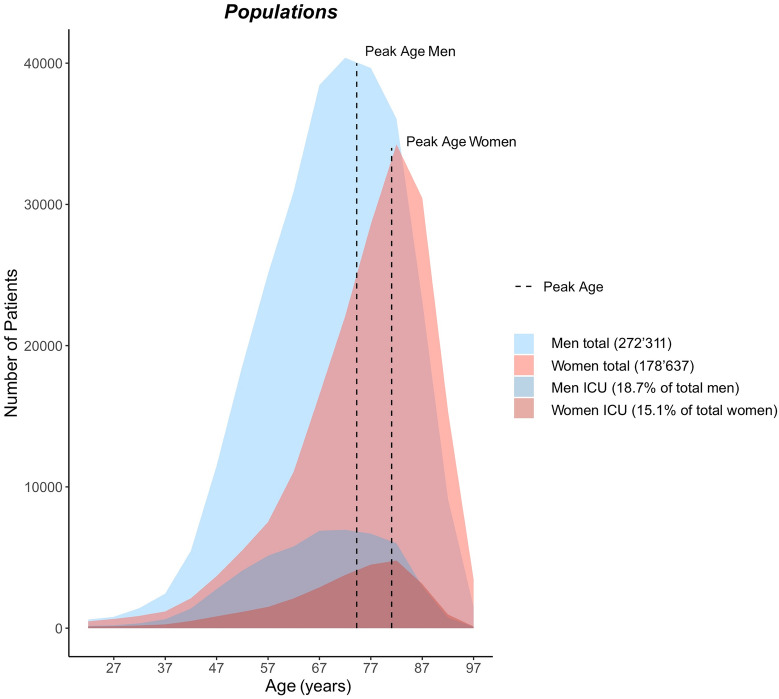
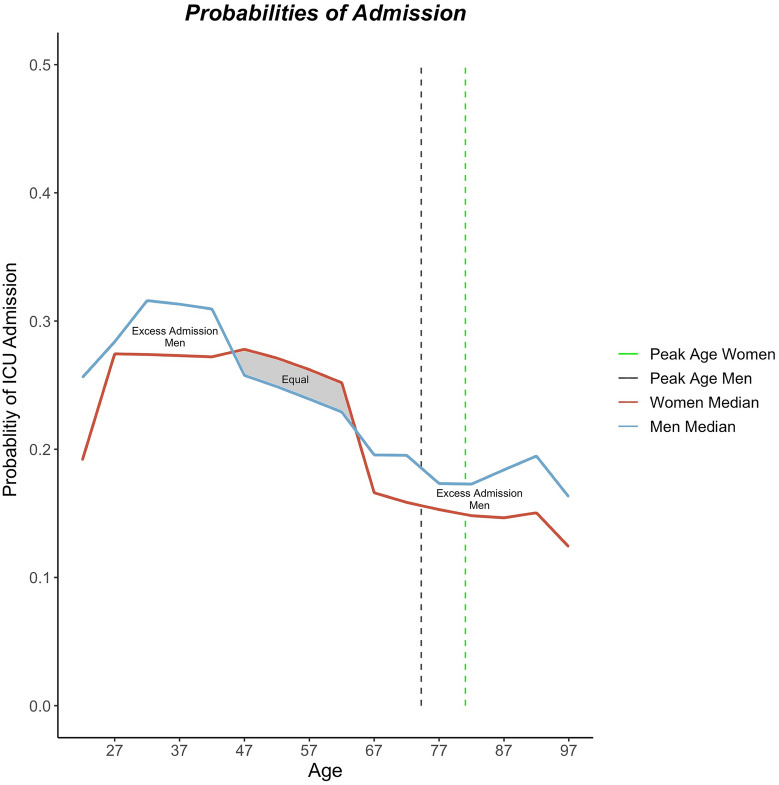
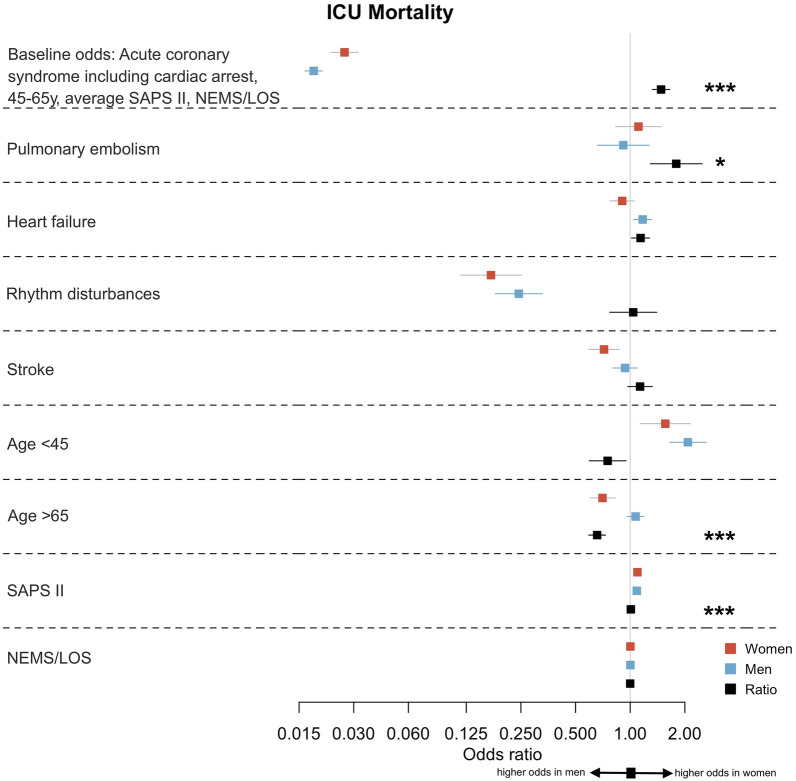
Results: For all diagnoses and populations, median ages at admission were consistently higher for women than for men [75 (64;82) years in women vs. 68 (58;77) years in men, p < 0.001]. Overall, women had a lower likelihood to be admitted to an intensive care unit (ICU) than men, despite being more severely ill [odds ratio (OR) 0.78 (0.76-0.79)]. ICU admission probability was lowest in women aged > 65 years (OR women:men 0.94 (0.89-0.99), p < 0.001). Women < 45 years had a similar ICU admission probability as men in the same age category [OR women:men 1.03 (0.94-1.13)], in spite of more severe illness. The odds to die were significantly higher in women than in men per unit increase in Simplified Acute Physiology Score (SAPS) II (OR 1.008 [1.004-1.012]).
Conclusion: In the care of the critically ill, our study suggests that women are less likely to receive ICU treatment regardless of disease severity. Underuse of ICU care was most prominent in younger women < 45 years. Although our study has several limitations that are imposed by the limited data available from the registries, our findings suggest that current ICU triage algorithms could benefit from careful reassessment. Further, and ideally prospective, studies are needed to confirm our findings.
Keywords: Cardiovascular disease; Critical illness; Gender bias; Survival; Women.
Conflict of interest statement
CG has received speakers’ fees from Sanofi Genzyme, travel support from Siemens Healthineers, and research support from the Novartis Foundation, Switzerland, and Bayer Pharmaceuticals. The Department of Nuclear Medicine, University Hospital Zurich, holds a research contract with GE Healthcare.
Figures
Comment in
-
Yentl syndrome and the ICU.Intensive Care Med. 2021 May;47(5):594-597. doi: 10.1007/s00134-021-06420-3. Epub 2021 May 5. Intensive Care Med. 2021. PMID: 33950371 No abstract available.
References
MeSH terms
Grants and funding
- CEG/Research Foundation in Anesthesiology and Intensive Care Medicine, University Hospital Basel
- CEG/Research Fund of the University of Basel
- CEG/Schweizerischer Nationalfonds zur Förderung der Wissenschaftlichen Forschung
- CG/Schweizerischer Nationalfonds zur Förderung der Wissenschaftlichen Forschung
- CG/Olga Mayenfisch Stiftung
- CG/OPO-Stiftung
- CG/Novartis Stiftung für Medizinisch-Biologische Forschung
- CG/Swissheart Foundation
- SB/Swissheart Foundation
- CG/Helmut Horten Foundation
- CG/EMDO Stiftung
- CG/Iten-Kohaut Foundation/University Hospital Zurich Foundation
- CG/LOOP-Zurich, Switzerland
- KA/Swiss Academy of Medical Sciences and the Gottfried and Julia Bangerter-Rhyner-Foundation, Switzerland
- SB/UZH Foundation, Switzerland
- AH/UZH Foundation
- RS/Swiss National Foundation (No 320030_169379)
- RS/Research Fund of the University Basel
- RS/Scientific Society Basel
- RS/Gottfried Julia Bangerter-Rhyner Foundation
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
