

Sex-Based Differences in COVID-19 Outcomes
- PMID: 33885345
- PMCID: PMC8182657
- DOI: 10.1089/jwh.2020.8974
Sex-Based Differences in COVID-19 Outcomes
Abstract
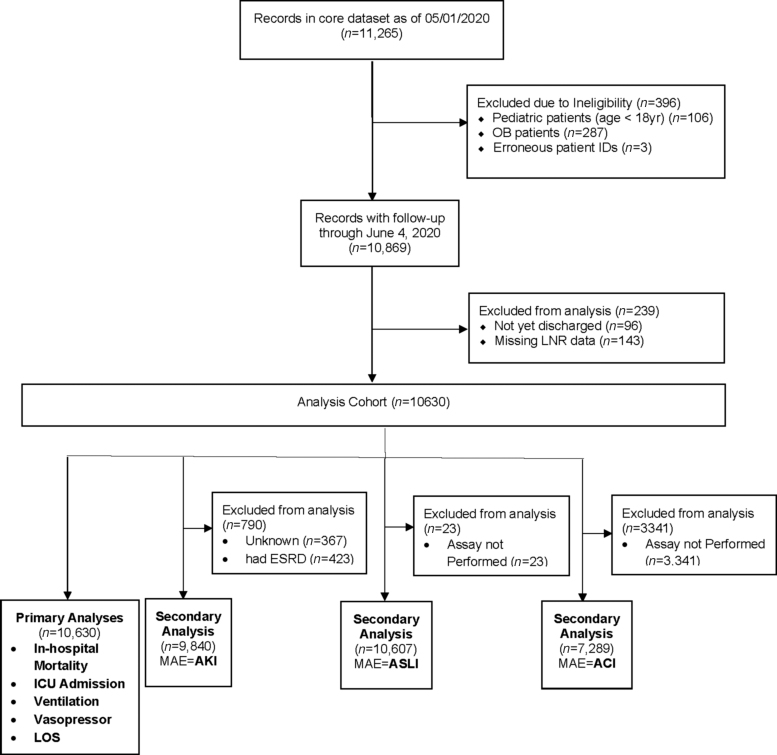
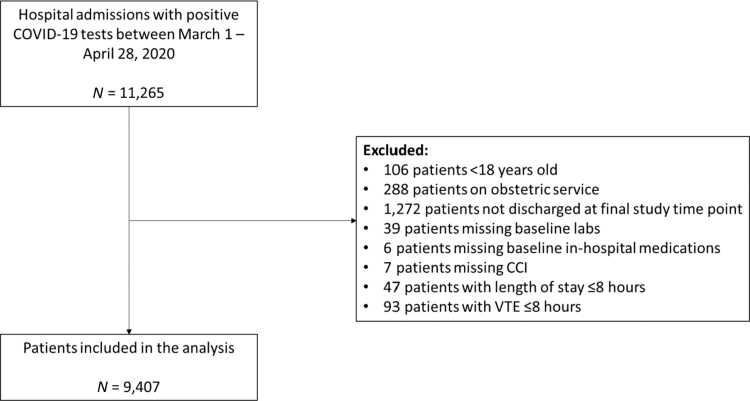
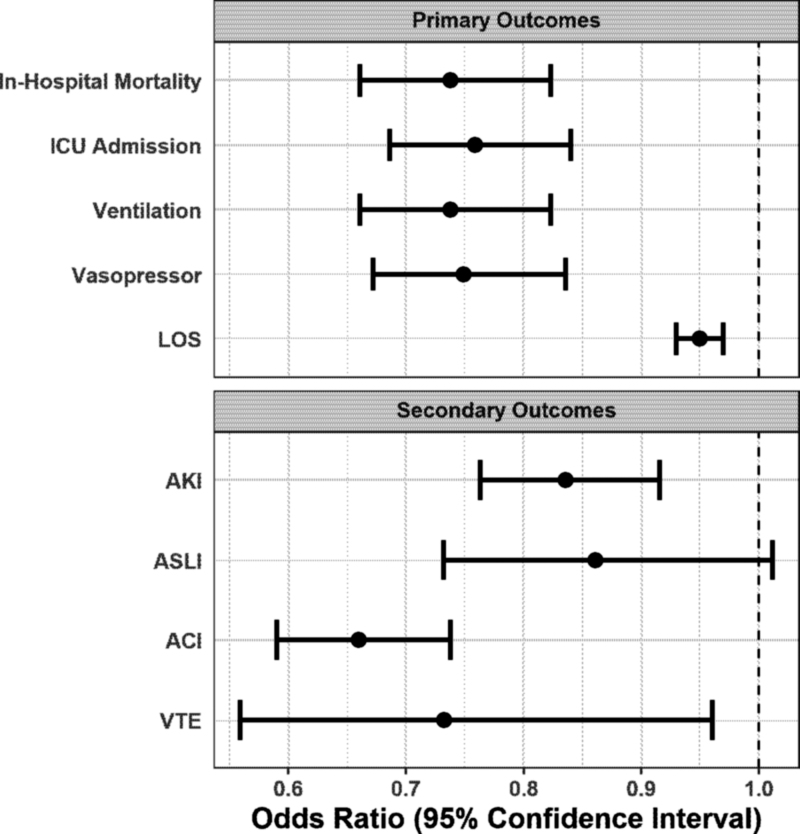
Background: Smaller studies suggest lower morbidity and mortality associated with coronavirus disease 2019 (COVID-19) in women. Our aim is to assess the impact of female sex on outcomes in a large cohort of patients hospitalized with COVID-19. Materials and Methods: This is a retrospective observational cohort study of 10,630 adult patients hospitalized with a confirmed COVID-19 polymerase chain reaction between March 1, 2020 and April 27, 2020, with follow-up conducted through June 4, 2020. Logistic regression was used to examine the relationship between sex and the primary outcomes, including length of stay, admission to intensive care unit (ICU), need for mechanical ventilation, pressor requirement, and all-cause mortality as well as major adverse events and in-hospital COVID-19 treatments. Results: In the multivariable analysis, women had 27% lower odds of in-hospital mortality (odds ratio [OR] = 0.73, 95% confidence interval [CI] 0.66-0.81; p < 0.001), 24% lower odds of ICU admission (OR = 0.76, 95% CI 0.69-0.84; p < 0.001), 26% lower odds of mechanical ventilation (OR = 0.74, 95% CI 0.66-0.82; p < 0.001), and 25% lower odds of vasopressor requirement (OR = 0.75, 95% CI 0.67-0.84; p < 0.001). Women had 34% less odds of having acute cardiac injury (OR = 0.66, 95% CI 0.59-0.74; p < 0.001; n = 7,289), 16% less odds of acute kidney injury (OR = 0.84, 95% CI 0.76-0.92; p < 0.001; n = 9,840), and 27% less odds of venous thromboembolism (OR = 0.73, 95% CI 0.56-0.96; p < 0.02; c-statistic 0.85, n = 9,407). Conclusions: Female sex is associated with lower odds of in-hospital outcomes, major adverse events, and all-cause mortality. There may be protective mechanisms inherent to female sex, which explain differences in COVID-19 outcomes.
Keywords: COVID-19; gender; hospital outcomes; intensive care; mortality; sex.
Conflict of interest statement
No competing financial interests exist.
Figures
Comment in
-
Lessons Learned from Coronavirus Disease 2019 Sex Disparities.J Womens Health (Larchmt). 2021 Apr;30(4):453-454. doi: 10.1089/jwh.2021.0110. Epub 2021 Mar 30. J Womens Health (Larchmt). 2021. PMID: 33784474 No abstract available.
References
-
- COVID-19 United States Cases by County. Johns Hopkins Coronavirus Resource Center. Available at: https://coronavirus.jhu.edu/us-map Accessed December9, 2020
-
- New York Covid Map and Case Count—The New York Times. Available at: https://www.nytimes.com/interactive/2020/us/new-york-coronavirus-cases.html Accessed December9, 2020
-
- Di Stadio A, Ricci G, Greco A, de Vincentiis M, Ralli M. Mortality rate and gender differences in COVID-19 patients dying in Italy: A comparison with other countries. Eur Rev Med Pharmacol Sci 2020;24:4066–4067 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
