

Using genetic variants to evaluate the causal effect of cholesterol lowering on head and neck cancer risk: A Mendelian randomization study
- PMID: 33886544
- PMCID: PMC8096036
- DOI: 10.1371/journal.pgen.1009525
Using genetic variants to evaluate the causal effect of cholesterol lowering on head and neck cancer risk: A Mendelian randomization study
Abstract
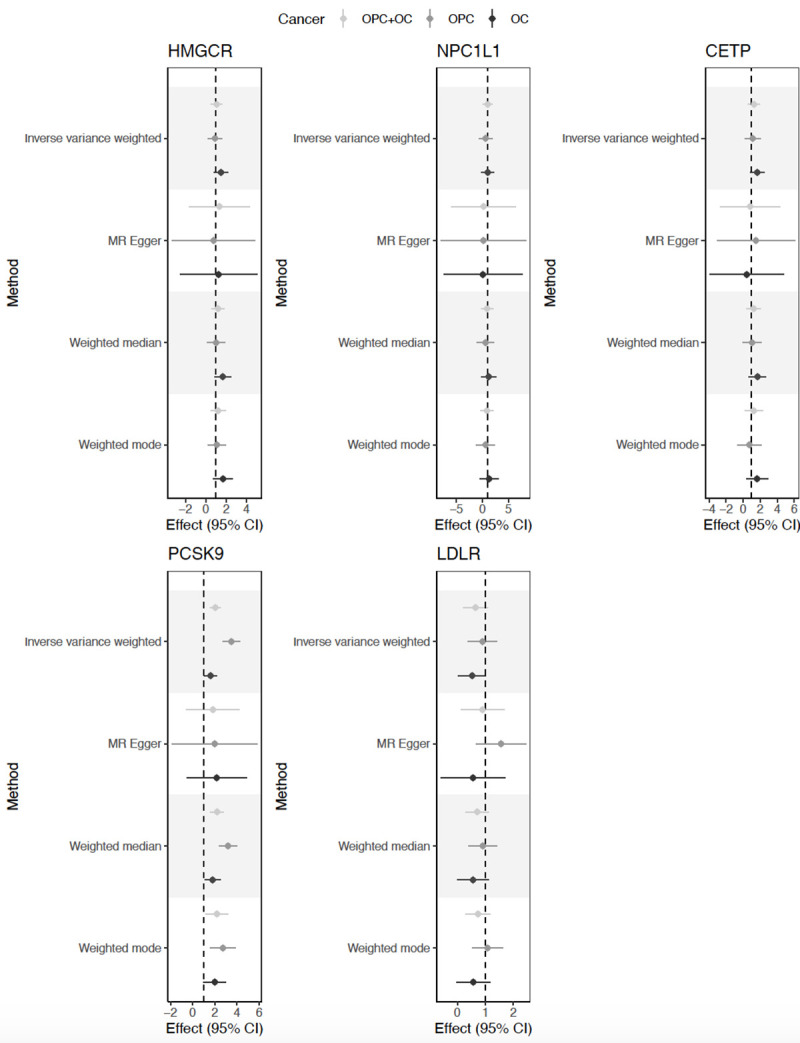
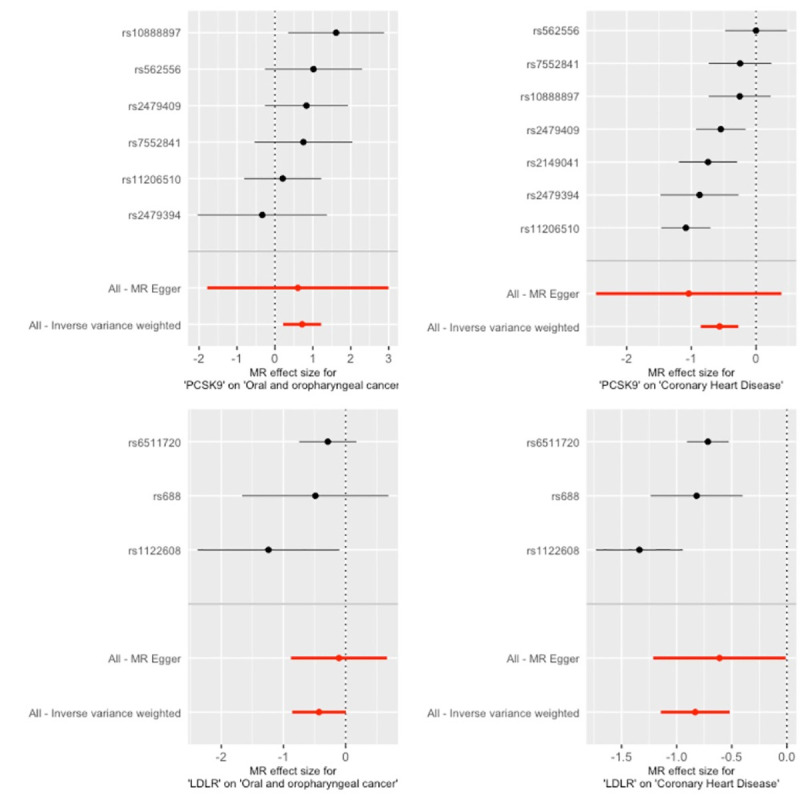
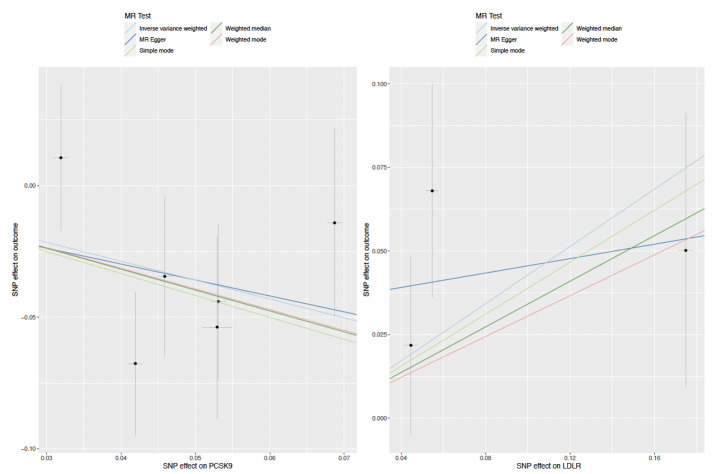
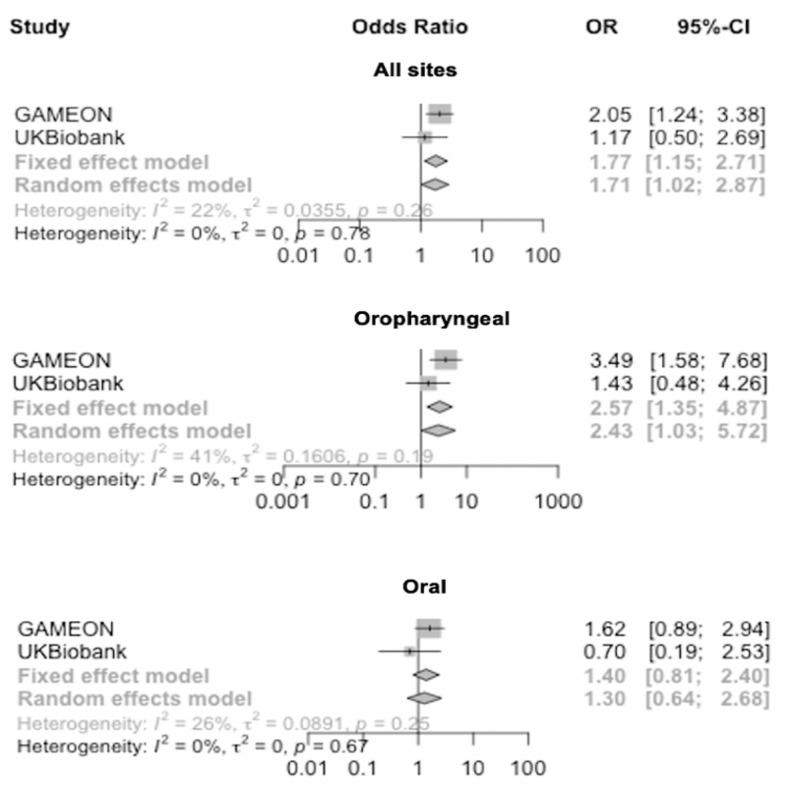
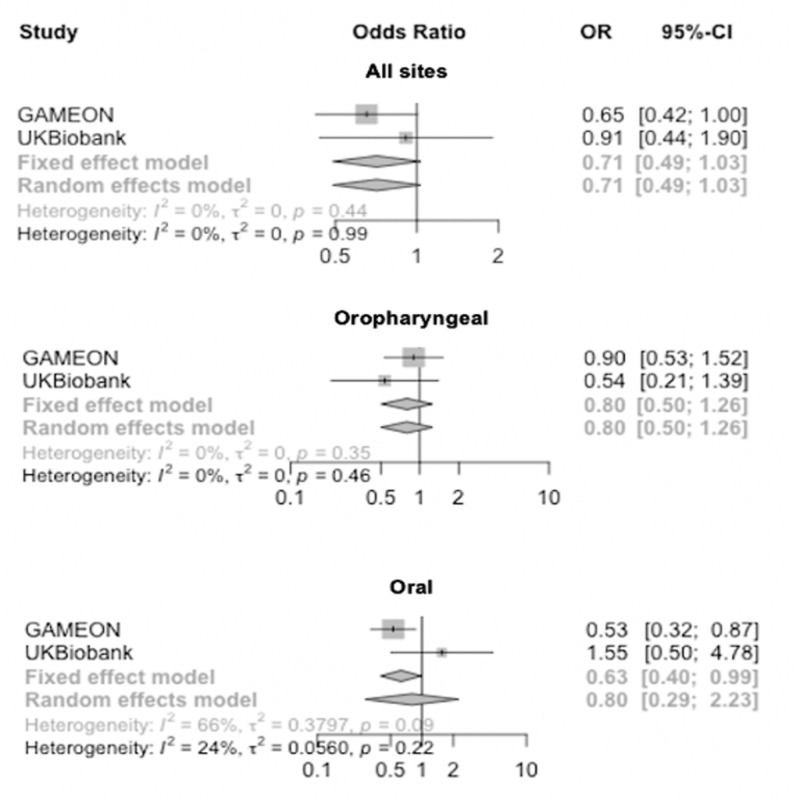
Head and neck squamous cell carcinoma (HNSCC), which includes cancers of the oral cavity and oropharynx, is a cause of substantial global morbidity and mortality. Strategies to reduce disease burden include discovery of novel therapies and repurposing of existing drugs. Statins are commonly prescribed for lowering circulating cholesterol by inhibiting HMG-CoA reductase (HMGCR). Results from some observational studies suggest that statin use may reduce HNSCC risk. We appraised the relationship of genetically-proxied cholesterol-lowering drug targets and other circulating lipid traits with oral (OC) and oropharyngeal (OPC) cancer risk using two-sample Mendelian randomization (MR). For the primary analysis, germline genetic variants in HMGCR, NPC1L1, CETP, PCSK9 and LDLR were used to proxy the effect of low-density lipoprotein cholesterol (LDL-C) lowering therapies. In secondary analyses, variants were used to proxy circulating levels of other lipid traits in a genome-wide association study (GWAS) meta-analysis of 188,578 individuals. Both primary and secondary analyses aimed to estimate the downstream causal effect of cholesterol lowering therapies on OC and OPC risk. The second sample for MR was taken from a GWAS of 6,034 OC and OPC cases and 6,585 controls (GAME-ON). Analyses were replicated in UK Biobank, using 839 OC and OPC cases and 372,016 controls and the results of the GAME-ON and UK Biobank analyses combined in a fixed-effects meta-analysis. We found limited evidence of a causal effect of genetically-proxied LDL-C lowering using HMGCR, NPC1L1, CETP or other circulating lipid traits on either OC or OPC risk. Genetically-proxied PCSK9 inhibition equivalent to a 1 mmol/L (38.7 mg/dL) reduction in LDL-C was associated with an increased risk of OC and OPC combined (OR 1.8 95%CI 1.2, 2.8, p = 9.31 x10-05), with good concordance between GAME-ON and UK Biobank (I2 = 22%). Effects for PCSK9 appeared stronger in relation to OPC (OR 2.6 95%CI 1.4, 4.9) than OC (OR 1.4 95%CI 0.8, 2.4). LDLR variants, resulting in genetically-proxied reduction in LDL-C equivalent to a 1 mmol/L (38.7 mg/dL), reduced the risk of OC and OPC combined (OR 0.7, 95%CI 0.5, 1.0, p = 0.006). A series of pleiotropy-robust and outlier detection methods showed that pleiotropy did not bias our findings. We found limited evidence for a role of cholesterol-lowering in OC and OPC risk, suggesting previous observational results may have been confounded. There was some evidence that genetically-proxied inhibition of PCSK9 increased risk, while lipid-lowering variants in LDLR, reduced risk of combined OC and OPC. This result suggests that the mechanisms of action of PCSK9 on OC and OPC risk may be independent of its cholesterol lowering effects; however, this was not supported uniformly across all sensitivity analyses and further replication of this finding is required.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Saba NF, Goodman M, Ward K, Flowers C, Ramalingam S, Owonikoko T, et al. Gender and ethnic disparities in incidence and survival of squamous cell carcinoma of the oral tongue, base of tongue, and tonsils: a surveillance, epidemiology and end results program-based analysis. Oncology. 2011;81(1):12–20. 10.1159/000330807 - DOI - PMC - PubMed
-
- Cancer Research UK (CRUK). Head and neck cancer statistics 2019. [cited 2019 11/04/2019]. Available from: https://www.cancerresearchuk.org/health-professional/cancer-statistics/s....
Publication types
MeSH terms
Substances
Grants and funding
- P30 ES010126/ES/NIEHS NIH HHS/United States
- MC_QA137853/MRC_/Medical Research Council/United Kingdom
- P30 CA047904/CA/NCI NIH HHS/United States
- MC_UU_00011/7/MRC_/Medical Research Council/United Kingdom
- MC_UU_00011/1/MRC_/Medical Research Council/United Kingdom
- 220530/Z/20/Z/WT_/Wellcome Trust/United Kingdom
- R01 CA090731/CA/NCI NIH HHS/United States
- RP-PG-0707-10034/DH_/Department of Health/United Kingdom
- MC_UU_00011/7/MRC_/Medical Research Council/United Kingdom
- C68933/A28534/CRUK_/Cancer Research UK/United Kingdom
- WT_/Wellcome Trust/United Kingdom
- MC_PC_17228/MRC_/Medical Research Council/United Kingdom
- 001/WHO_/World Health Organization/International
- 29019/CRUK_/Cancer Research UK/United Kingdom
- P30 CA016086/CA/NCI NIH HHS/United States
- C18281/A29019/CRUK_/Cancer Research UK/United Kingdom
- R01 DE025712/DE/NIDCR NIH HHS/United States
- C18281/A19169/CRUK_/Cancer Research UK/United Kingdom
- P50 CA097190/CA/NCI NIH HHS/United States
- 28534/CRUK_/Cancer Research UK/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
