

Extracorporeal membrane oxygenation network organisation and clinical outcomes during the COVID-19 pandemic in Greater Paris, France: a multicentre cohort study
- PMID: 33887246
- PMCID: PMC8055207
- DOI: 10.1016/S2213-2600(21)00096-5
Extracorporeal membrane oxygenation network organisation and clinical outcomes during the COVID-19 pandemic in Greater Paris, France: a multicentre cohort study
Erratum in
-
Correction to Lancet Respir Med 2021; published online April 19. https://doi.org/10.1016/S2213-2600(21)00096-5.Lancet Respir Med. 2021 Jun;9(6):e55. doi: 10.1016/S2213-2600(21)00209-5. Epub 2021 Apr 27. Lancet Respir Med. 2021. PMID: 33915102 Free PMC article. No abstract available.
-
Correction to Lancet Respir Med 2021; published online April 19. https://doi.org/10.1016/S2213-2600(21)00096-5.Lancet Respir Med. 2021 Jul;9(7):e62. doi: 10.1016/S2213-2600(21)00280-0. Lancet Respir Med. 2021. PMID: 34214501 Free PMC article. No abstract available.
Abstract
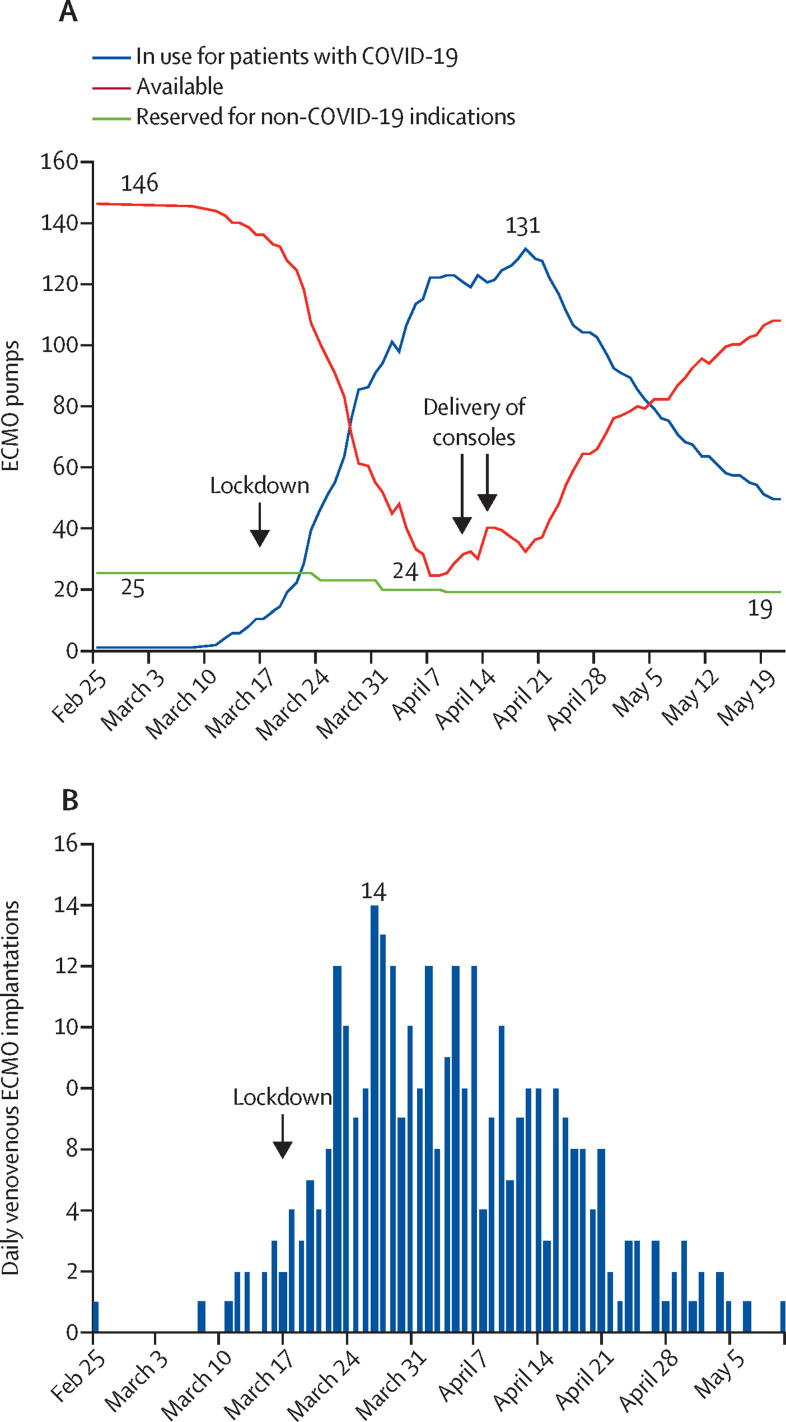
Background: In the Île-de-France region (henceforth termed Greater Paris), extracorporeal membrane oxygenation (ECMO) for severe acute respiratory distress syndrome (ARDS) was considered early in the COVID-19 pandemic. We report ECMO network organisation and outcomes during the first wave of the pandemic.
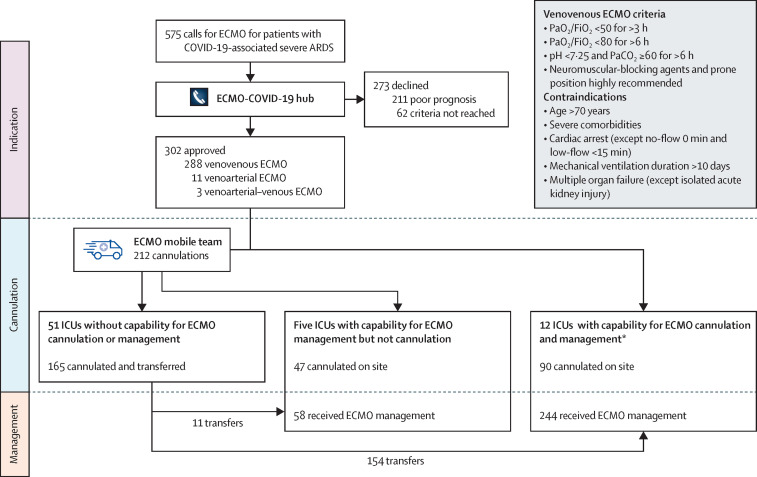
Methods: In this multicentre cohort study, we present an analysis of all adult patients with laboratory-confirmed SARS-CoV-2 infection and severe ARDS requiring ECMO who were admitted to 17 Greater Paris intensive care units between March 8 and June 3, 2020. Central regulation for ECMO indications and pooling of resources were organised for the Greater Paris intensive care units, with six mobile ECMO teams available for the region. Details of complications (including ECMO-related complications, renal replacement therapy, and pulmonary embolism), clinical outcomes, survival status at 90 days after ECMO initiation, and causes of death are reported. Multivariable analysis was used to identify pre-ECMO variables independently associated with 90-day survival after ECMO.
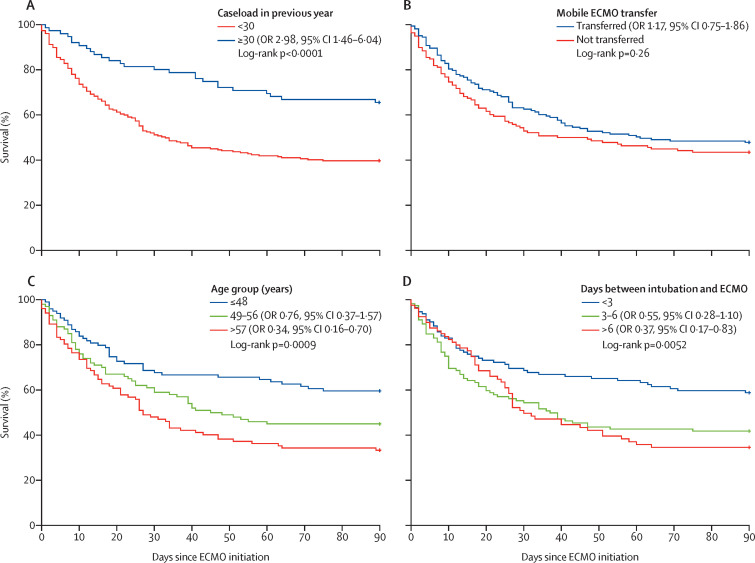
Findings: The 302 patients included who underwent ECMO had a median age of 52 years (IQR 45-58) and Simplified Acute Physiology Score-II of 40 (31-56), and 235 (78%) of whom were men. 165 (55%) were transferred after cannulation by a mobile ECMO team. Before ECMO, 285 (94%) patients were prone positioned, median driving pressure was 18 cm H2O (14-21), and median ratio of the partial pressure of arterial oxygen to the fraction of inspired oxygen was 61 mm Hg (IQR 54-70). During ECMO, 115 (43%) of 270 patients had a major bleeding event, 27 of whom had intracranial haemorrhage; 130 (43%) of 301 patients received renal replacement therapy; and 53 (18%) of 294 had a pulmonary embolism. 138 (46%) patients were alive 90 days after ECMO. The most common causes of death were multiorgan failure (53 [18%] patients) and septic shock (47 [16%] patients). Shorter time between intubation and ECMO (odds ratio 0·91 [95% CI 0·84-0·99] per day decrease), younger age (2·89 [1·41-5·93] for ≤48 years and 2·01 [1·01-3·99] for 49-56 years vs ≥57 years), lower pre-ECMO renal component of the Sequential Organ Failure Assessment score (0·67, 0·55-0·83 per point increase), and treatment in centres managing at least 30 venovenous ECMO cases annually (2·98 [1·46-6·04]) were independently associated with improved 90-day survival. There was no significant difference in survival between patients who had mobile and on-site ECMO initiation.
Interpretation: Beyond associations with similar factors to those reported on ECMO for non-COVID-19 ARDS, 90-day survival among ECMO-assisted patients with COVID-19 was strongly associated with a centre's experience in venovenous ECMO during the previous year. Early ECMO management in centres with a high venovenous ECMO case volume should be advocated, by applying centralisation and regulation of ECMO indications, which should also help to prevent a shortage of resources.
Funding: None.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests GL reports lecture fees from Livanova and Abiomed, outside of the submitted work. MS reports lecture fees from Getinge, Dräger, and Xenios, outside of the submitted work. BC reports consulting and lecture fees from Edwards Lifesciences, Orion Pharma, Amomed, and Nordic Pharma, outside of the submitted work. RS has received lecture fees from Baxter, outside of the submitted work. DL reports speaker fees and is a member of advisory boards for Edwards Lifesciences, Medtronic, and Masimo, outside of the submitted work. AC reports grants and personal fees from Getinge, and personal fees from Baxter and Xenios, outside of the submitted work. All other authors declare no competing interests.
Figures
Comment in
-
COVID-19 and ECMO: a call for close cooperation and more investigation.Lancet Respir Med. 2021 Aug;9(8):805-807. doi: 10.1016/S2213-2600(21)00128-4. Epub 2021 Apr 19. Lancet Respir Med. 2021. PMID: 33887245 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
