

Prospective experimental treatment of colorectal cancer patients based on organoid drug responses
- PMID: 33887686
- PMCID: PMC8086019
- DOI: 10.1016/j.esmoop.2021.100103
Prospective experimental treatment of colorectal cancer patients based on organoid drug responses
Abstract
Background: Organoid technology has recently emerged as a powerful tool to assess drug sensitivity of individual patient tumors in vitro. Organoids may therefore represent a new avenue for precision medicine, as this circumvents many of the complexities associated with DNA- or transcriptional-profiling.
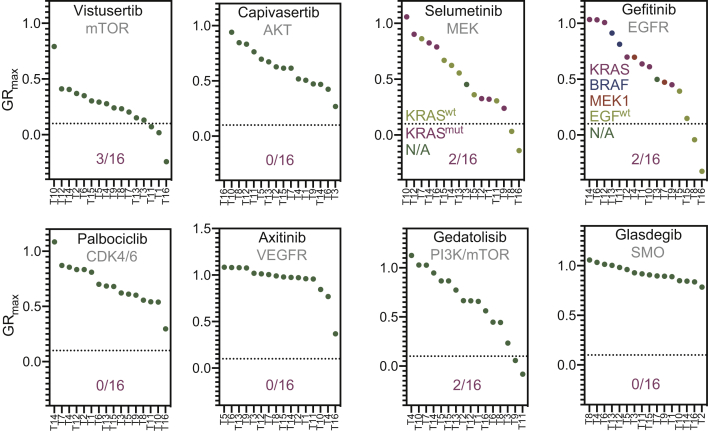
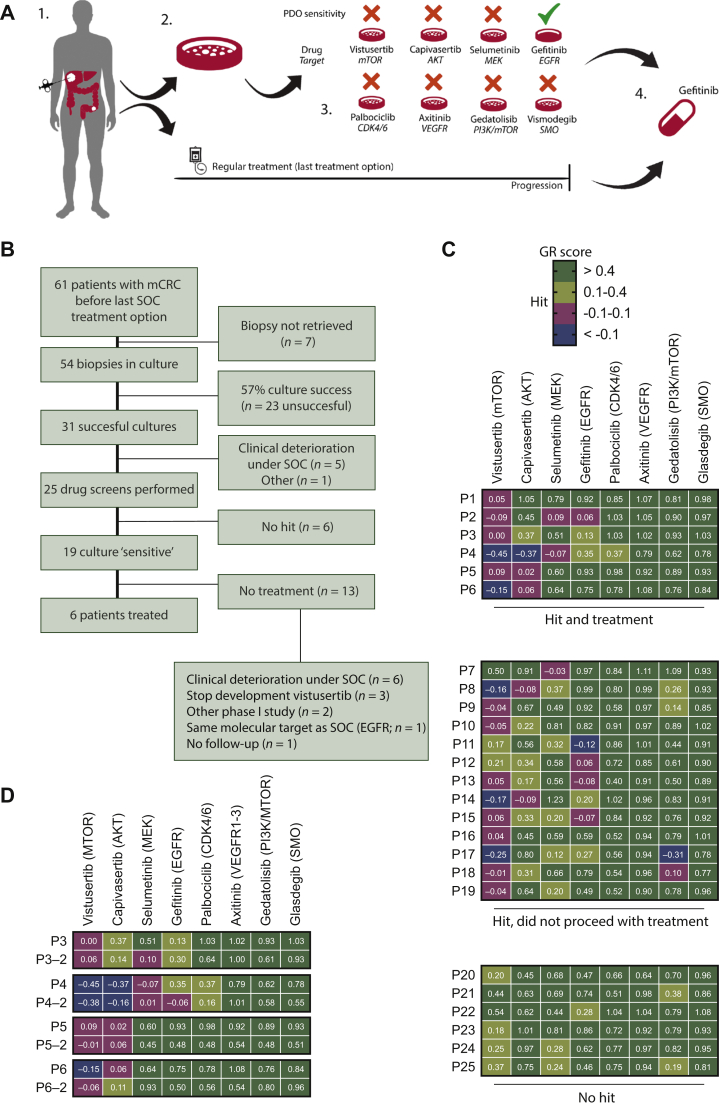
Materials and methods: The SENSOR trial was a single-arm, single-center, prospective intervention trial to evaluate the feasibility of patient-derived organoids to allocate patients for treatment with off-label or investigational agents. The primary endpoint was an objective response rate of ≥20%. Patients underwent a biopsy for culture before commencing their last round standard of care. Organoids were exposed to a panel of eight drugs and patients were treated after progression on standard-of-care treatment and when a clear signal of antitumor activity was identified in vitro.
Results: Sixty-one patients were included and we generated 31 organoids of 54 eligible patients. Twenty-five cultures were subjected to drug screening and 19 organoids exhibited substantial responses to one or more drugs. Three patients underwent treatment with vistusertib and three with capivasertib. Despite drug sensitivity of organoids, patients did not demonstrate objective clinical responses to the recommended treatment.
Conclusions: Organoid technology had limited value as a tool for precision medicine in this patient population because a large fraction of patients could not undergo treatment or because the recommended treatment did not elicit an objective response. We identified several essential parameters, such as the culture success rate, clinical deterioration of patients during standard of care, and rational design of drug panels that need to be accounted for in organoid-guided clinical studies.
Keywords: clinical trial; colorectal cancer; drug screening; experimental treatment; precision medicine; tumor organoids.
Copyright © 2021 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Disclosure EEV is the medical director of The Netherlands Cancer Institute and legally responsible for all contracts with AstraZeneca and Pfizer. AstraZeneca and Pfizer provided compounds for drug screening and patient treatment. All other authors have declared no conflicts of interest. Data sharing Reagents used under material transfer agreement (MTA) are Wnt-3a, Noggin (Hans Clevers, Hubrecht Institute), and R-spondin-1 producer lines (Calvin Kuo, Stanford). DNA sequencing data for T1, T5, T6, and T8 is published in the manuscript by Wetering et al. Cell, 2015.(8) WGS data is published and deposited by Priestley et al. Nature, 2019.(33) Deposition of targeted-sequencing data and distribution of organoids and deposition of DNA sequencing data in publicly available databases are regulated by the informed consent that participants to this study signed. All materials and data on a per-patient level can be obtained through the Institutional Review Board of The Netherlands Cancer Institute (IRB@nki.nl). All other materials used in this study are freely or commercially available.
Figures
References
-
- Le Tourneau C., Delord J.P., Goncalves A. Molecularly targeted therapy based on tumour molecular profiling versus conventional therapy for advanced cancer (SHIVA): a multicentre, open-label, proof-of-concept, randomised, controlled phase 2 trial. Lancet Oncol. 2015;16(13):1324–1334. - PubMed
-
- van der Velden D.L., Hoes L.R., van der Wijngaart H. The Drug Rediscovery protocol facilitates the expanded use of existing anticancer drugs. Nature. 2019;574(7776):127–131. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
