

Recommendations for respiratory syncytial virus surveillance at the national level
- PMID: 33888523
- PMCID: PMC8485062
- DOI: 10.1183/13993003.03766-2020
Recommendations for respiratory syncytial virus surveillance at the national level
Abstract
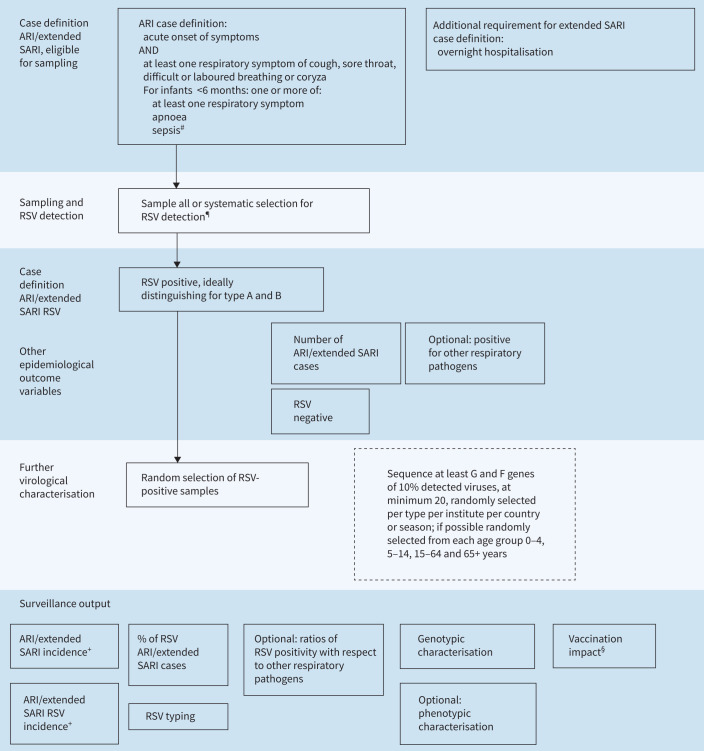
Respiratory syncytial virus (RSV) is a common cause of acute lower respiratory tract infections and hospitalisations among young children and is globally responsible for many deaths in young children, especially in infants aged <6 months. Furthermore, RSV is a common cause of severe respiratory disease and hospitalisation among older adults. The development of new candidate vaccines and monoclonal antibodies highlights the need for reliable surveillance of RSV. In the European Union (EU), no up-to-date general recommendations on RSV surveillance are currently available. Based on outcomes of a workshop with 29 European experts in the field of RSV virology, epidemiology and public health, we provide recommendations for developing a feasible and sustainable national surveillance strategy for RSV that will enable harmonisation and data comparison at the European level. We discuss three surveillance components: active sentinel community surveillance, active sentinel hospital surveillance and passive laboratory surveillance, using the EU acute respiratory infection and World Health Organization (WHO) extended severe acute respiratory infection case definitions. Furthermore, we recommend the use of quantitative reverse transcriptase PCR-based assays as the standard detection method for RSV and virus genetic characterisation, if possible, to monitor genetic evolution. These guidelines provide a basis for good quality, feasible and affordable surveillance of RSV. Harmonisation of surveillance standards at the European and global level will contribute to the wider availability of national level RSV surveillance data for regional and global analysis, and for estimation of RSV burden and the impact of future immunisation programmes.
Copyright ©The authors 2021.
Conflict of interest statement
Conflict of Interest: A.C. Teirlinck reports grants from Innovative Medicines Initiative, during the conduct of the study. Conflict of interest: E.K. Broberg has nothing to disclose. Conflict of interest: A. Stuwitz Berg has nothing to disclose. Conflict of interest: H. Campbell reports grants from Innovative Medicines Initiative, and grants and personal fees (paid via the university) from WHO, Bill and Melinda Gates Foundation and Sanofi, during the conduct of the study. Conflict of interest: R.M. Reeves reports grants from Innovative Medicines Initiative, during the conduct of the study. Conflict of interest: A. Carnahan has nothing to disclose. Conflict of interest: B. Lina has nothing to disclose. Conflict of interest: G. Pakarna has nothing to disclose. Conflict of interest: H. Bøås has nothing to disclose. Conflict of interest: H. Nohynek reports grants from GSK, SanofiPasteur and Pfizer (to their institute THL, not their unit), outside the submitted work; and membership of the ESWI Scientific Committee. Conflict of interest: H-D. Emborg reports grants from Innovative Medicines Initiative (grant agreement 116019), during the conduct of the study. Conflict of interest: H. Nair reports grants from Innovative Medicines Initiative, during the conduct of the study; grants and personal fees from Bill and Melinda Gates Foundation, World Health Organization and Sanofi, and personal fees from Janssen and Abbvie, outside the submitted work. Conflict of interest: J. Reiche has nothing to disclose. Conflict of interest: J.A. Oliva has nothing to disclose. Conflict of interest: J.O. Gorman has nothing to disclose. Conflict of interest: J. Paget reports grants from Sanofi Pasteur, WHO, and Foundation for Influenza Epidemiology, outside the submitted work. Conflict of interest: K. Szymański has nothing to disclose. Conflict of interest: K. Danis has nothing to disclose. Conflict of interest: M. Socan has nothing to disclose. Conflict of interest: M. Gijon has nothing to disclose. Conflict of interest: M. Rapp has nothing to disclose. Conflict of interest: R. Trebbien reports grants from Innovative Medicines Initiative, during the conduct of the study. Conflict of interest: R. Guiomar has nothing to disclose. Conflict of interest: S.S. Hirve has nothing to disclose. Conflict of interest: S. Buda has nothing to disclose. Conflict of interest: S. van der Werf reports non-financial support from RESCEU (travel and hotel costs to attend the workshop on RSV surveillance), during the conduct of the study and is a Board member of ISIRV. Conflict of interest: A. Meijer reports grants from Innovative Medicines Initiative, during the conduct of the study. Conflict of interest: T.K. Fischer has nothing to disclose.
Figures
References
-
- Shi T, McAllister DA, O'Brien KL, et al. . Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet 2017; 390: 946–958. doi:10.1016/S0140-6736(17)30938-8 - DOI - PMC - PubMed
-
- Glezen WP, Taber LH, Frank AL, et al. . Risk of primary infection and reinfection with respiratory syncytial virus. Am J Dis Child 1986; 140: 543–546. - PubMed
-
- Shi T, Ooi Y, Zaw EM, et al. . Association between respiratory syncytial virus-associated acute lower respiratory infection in early life and recurrent wheeze and asthma in later childhood. J Infect Dis 2020; 222: Suppl. 7, S628–S633. - PubMed
-
- Shi T, Denouel A, Tietjen AK, et al. . Global disease burden estimates of respiratory syncytial virus-associated acute respiratory infection in older adults in 2015: a systematic review and meta-analysis. J Infect Dis 2020; 222: Suppl. 7, S577–S583. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical