

Development and Validation of Risk Prediction Model for In-hospital Mortality Among Patients Hospitalized With Acute Exacerbation Chronic Obstructive Pulmonary Disease Between 2015 and 2019
- PMID: 33889584
- PMCID: PMC8055833
- DOI: 10.3389/fmed.2021.630870
Development and Validation of Risk Prediction Model for In-hospital Mortality Among Patients Hospitalized With Acute Exacerbation Chronic Obstructive Pulmonary Disease Between 2015 and 2019
Abstract
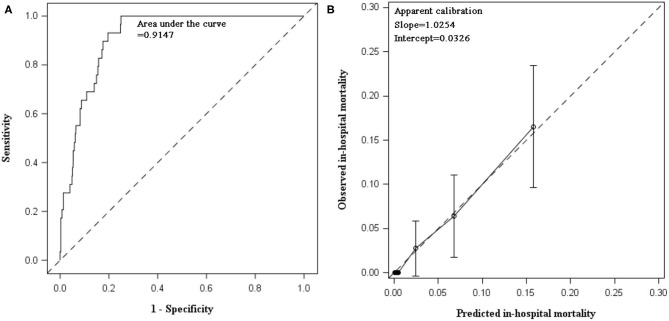
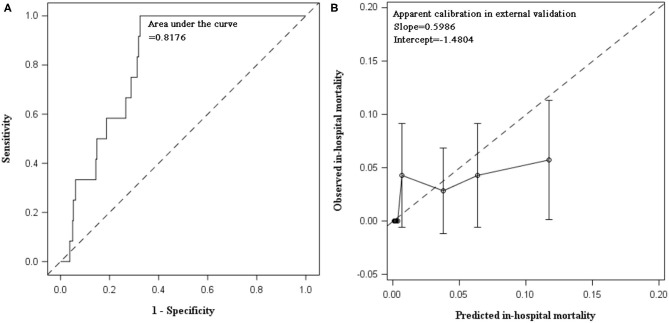
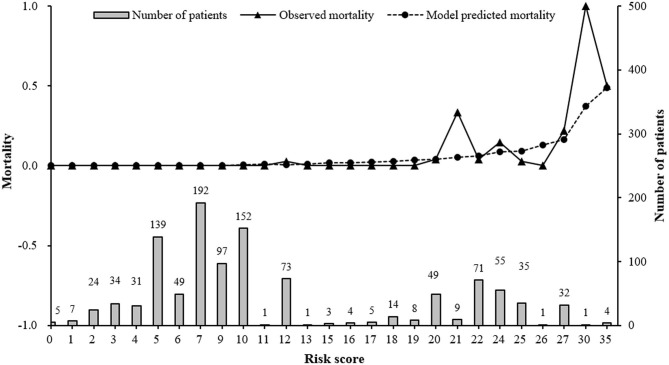
Background: In patients with chronic obstructive pulmonary disease (COPD), acute exacerbations affect patients' health and can lead to death. This study was aimed to develop a prediction model for in-hospital mortality in patients with acute exacerbations of COPD (AECOPD). Method: A retrospective study was performed in patients hospitalized for AECOPD between 2015 and 2019. Patients admitted between 2015 and 2017 were included to develop model and individuals admitted in the following 2 years were included for external validation. We analyzed variables that were readily available in clinical practice. Given that death was a rare outcome in this study, we fitted Firth penalized logistic regression. C statistic and calibration plot quantified the model performance. Optimism-corrected C statistic and slope were estimated by bootstrapping. Accordingly, the prediction model was adjusted and then transformed into risk score. Result: Between 2015 and 2017, 1,096 eligible patients were analyzed, with a mean age of 73 years and 67.8% male. The in-hospital mortality was 2.6%. Compared to survivors, non-survivors were older, more admitted from emergency, more frequently concomitant with respiratory failure, pneumothorax, hypoxic-hypercarbic encephalopathy, and had longer length of stay (LOS). Four variables were included into the final model: age, respiratory failure, pneumothorax, and LOS. In internal validation, C statistic was 0.9147, and the calibration slope was 1.0254. Their optimism-corrected values were 0.90887 and 0.9282, respectively, indicating satisfactory discrimination and calibration. When externally validated in 700 AECOPD patients during 2018 and 2019, the model demonstrated good discrimination with a C statistic of 0.8176. Calibration plot illustrated a varying discordance between predicted and observed mortality. It demonstrated good calibration in low-risk patients with predicted mortality rate ≤10% (P = 0.3253) but overestimated mortality in patients with predicted rate >10% (P < 0.0001). The risk score of 20 was regarded as a threshold with an optimal Youden index of 0.7154. Conclusion: A simple prediction model for AECOPD in-hospital mortality has been developed and externally validated. Based on available data in clinical setting, the model could serve as an easily used instrument for clinical decision-making. Complications emerged as strong predictors, underscoring an important role of disease management in improving patients' prognoses during exacerbation episodes.
Keywords: acute exacerbation of COPD; development; in-hospital mortality; prediction model; validation.
Copyright © 2021 Dong, Ren, Huang, Wang, Jiao and Yang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Global Burden of Disease Collaborative Network . Global Burden of Disease Study 2017 (GBD 2017) Results. Seattle: Institute for Health Metrics and Evaluation (IHME) (2018). Available online at: http://ghdx.healthdata.org/gbd-results-tool
LinkOut - more resources
Full Text Sources
Other Literature Sources