

Assessment of the Safety and Therapeutic Benefits of Convalescent Plasma in COVID-19 Treatment: A Systematic Review and Meta-Analysis
- PMID: 33889590
- PMCID: PMC8055850
- DOI: 10.3389/fmed.2021.660688
Assessment of the Safety and Therapeutic Benefits of Convalescent Plasma in COVID-19 Treatment: A Systematic Review and Meta-Analysis
Abstract
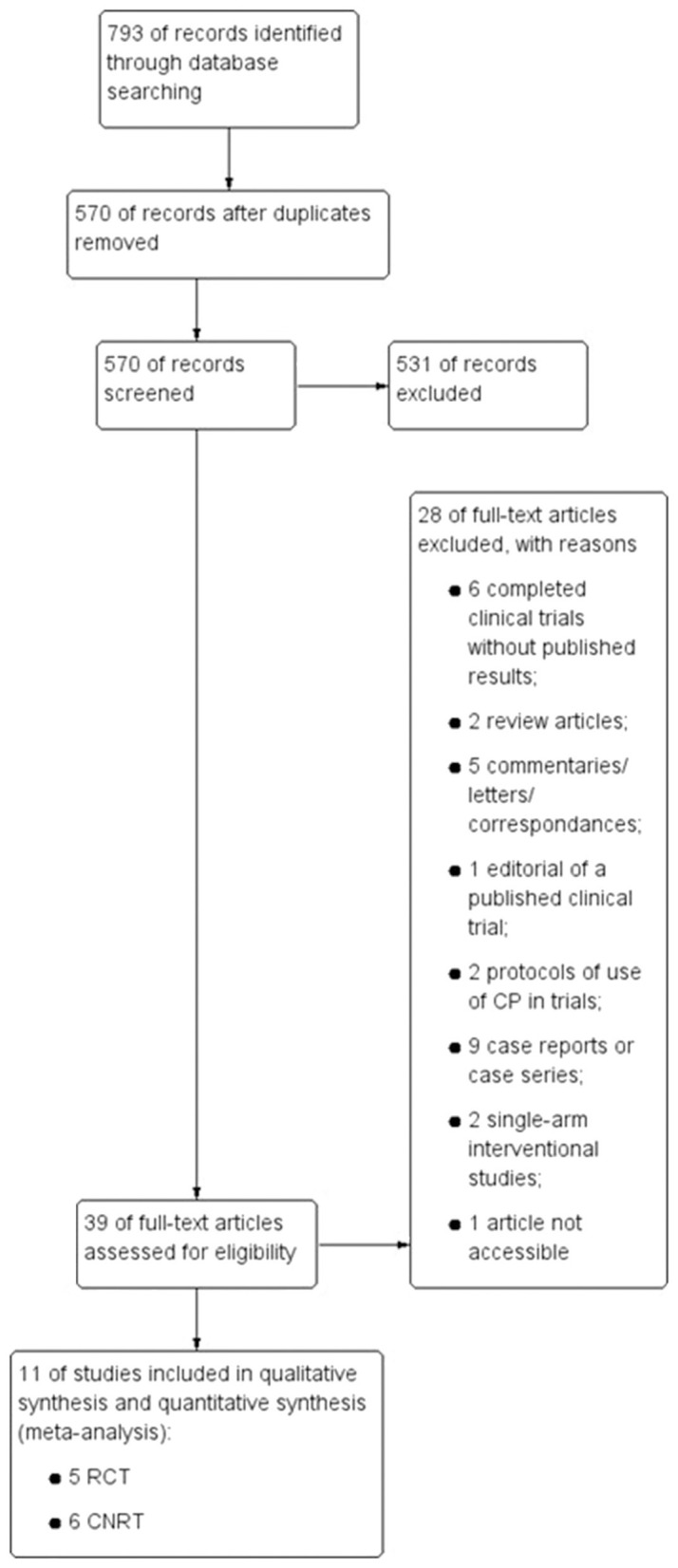
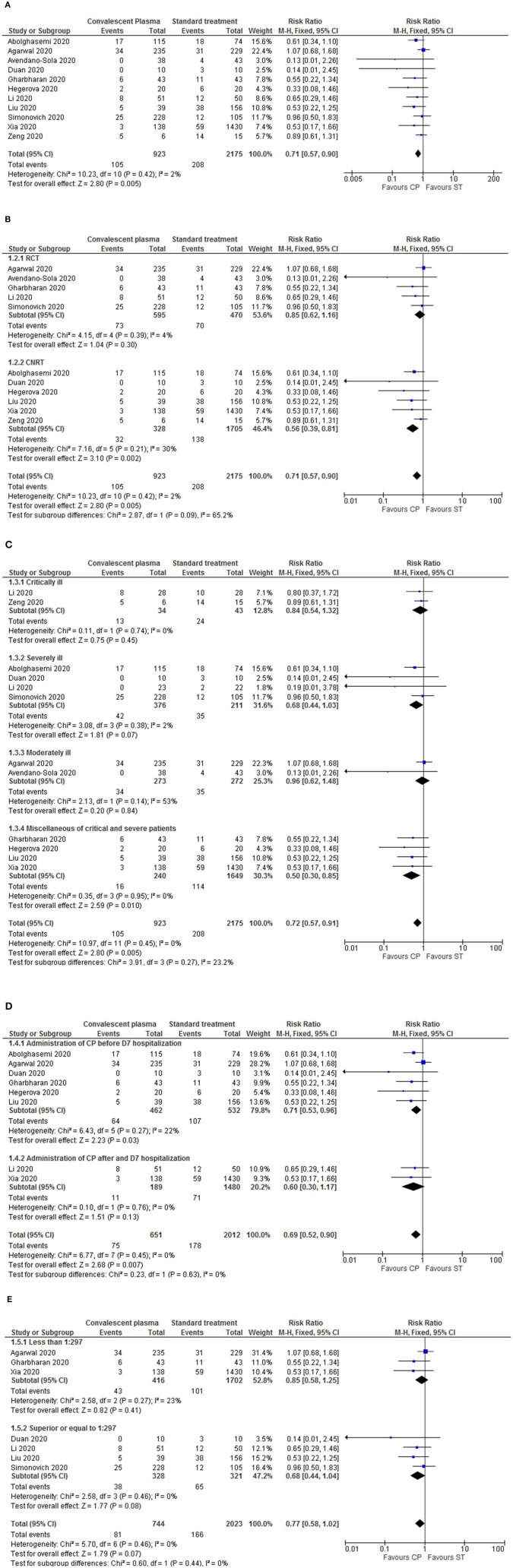
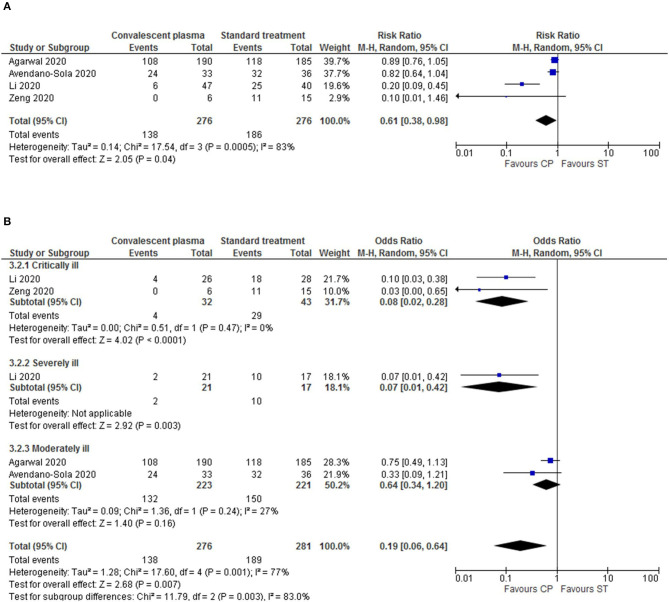
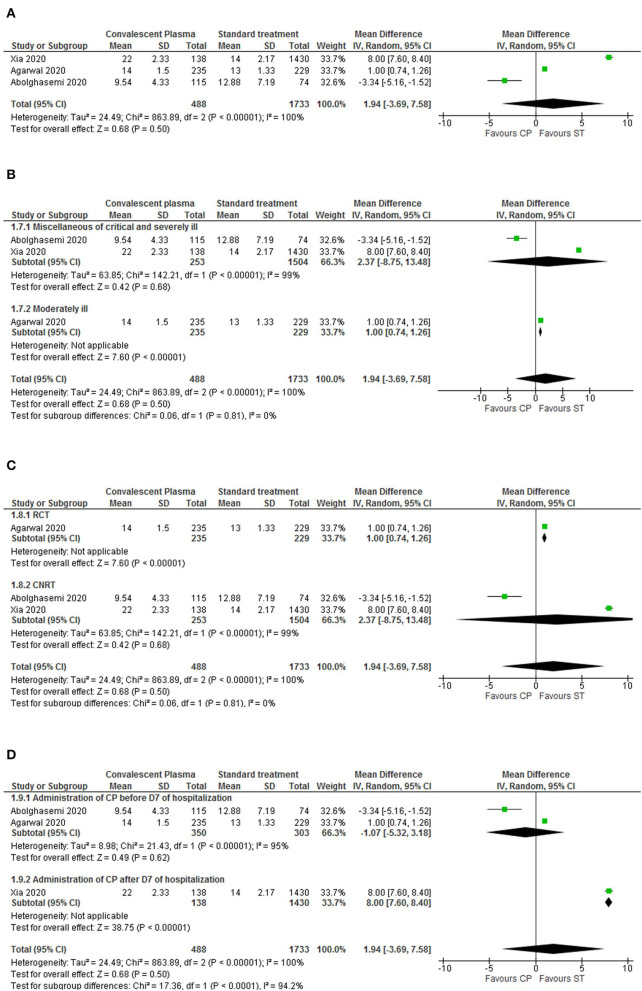
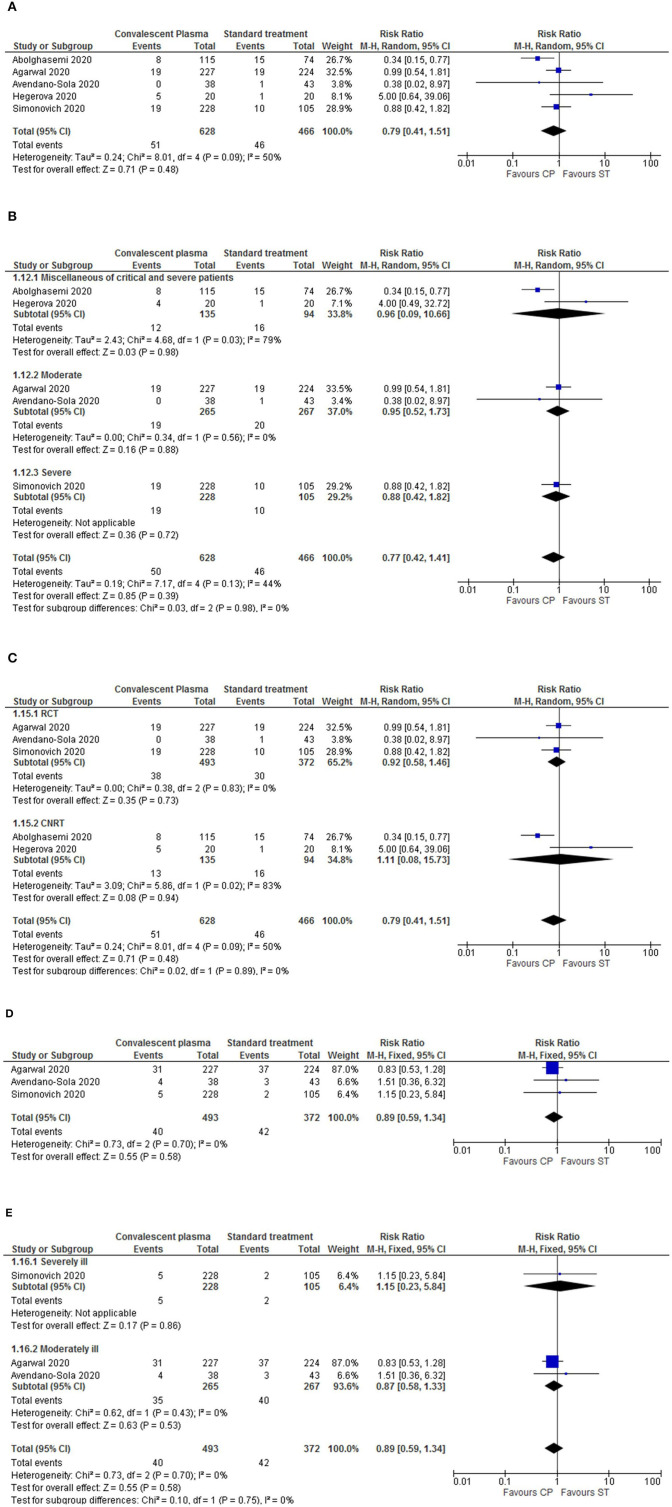
Background: The coronavirus disease (COVID-19), caused by the Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2), prompted a global health crisis, with no available specific treatments. Convalescent plasma (CP) with neutralizing antibodies could be a promising therapeutic approach to reduce mortality. Objectives: To evaluate the therapeutic potential of CP for COVID-19 and to assess its safety and efficacy in reducing the patients' mortality. Methods: We retrieved clinical trial references from multiple Databases (e.g., PubMed, B-On, SCOPUS), for complete studies until November 26th 2020. We included Randomized controlled trials (RCT) and controlled non-randomized trials (CNRT), that assessed the efficacy of CP to treat hospitalized COVID-19 patients. Trials were included regardless of concomitant medications in the intervention's arms. Eleven trials met our eligibility criteria. This study was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. We defined a methodological protocol to extract and evaluate all pertinent baseline demographics and interventions' characteristics from trials. The primary outcomes were the safety profile of CP, measured by the type, frequency and severity of adverse events, and CP effectiveness in reducing mortality, measured by the number of deaths registered for this therapy. Results: We assessed 11 trials (5 RCT and 6 CNRT) with 3,098 participants, of whom 923 patients were treated with CP. Only 32 (3.5%) of the treated patients suffered adverse events (from which 9.4% serious transfusion-related adverse events). The overall mortality rates were significantly decreased by CP administration {risk ratio (RR) 0.71, p = 0.005, 95% confidence interval (Cl) [0.57-0.90]}, with low heterogeneity. In the sub-analysis by period of transfusion, CP transfusion within a week of hospitalization contributed to diminished mortality rate (RR = 0.71, p = 0.03, 95%Cl [0.53-0.96]). CP therapy also led to significantly reduced viral loads at 72 h after transfusion (RR = 0.61, p = 0.04, 95%Cl [0.38-0.98]), despite high heterogeneity due to disease severity. Conclusion: This meta-analysis established CP as a safe and potentially effective therapy for COVID-19, decreasing the mortality rates and promoting a swift viral clearance. Further studies are necessary to provide stronger evidence.
Keywords: COVID-19; clinical trials; convalescent plasma; meta-analysis; mortality; safety; viral clearance.
Copyright © 2021 Barreira, Lourenço, Calisto, Moreira-Gonçalves, Santos and Videira.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Organization WH . Coronavirus Disease (COVID-19) Pandemic. (2020). Available online at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous