

Spatiotemporal dynamics between interictal epileptiform discharges and ripples during associative memory processing
- PMID: 33889945
- PMCID: PMC8219352
- DOI: 10.1093/brain/awab044
Spatiotemporal dynamics between interictal epileptiform discharges and ripples during associative memory processing
Abstract
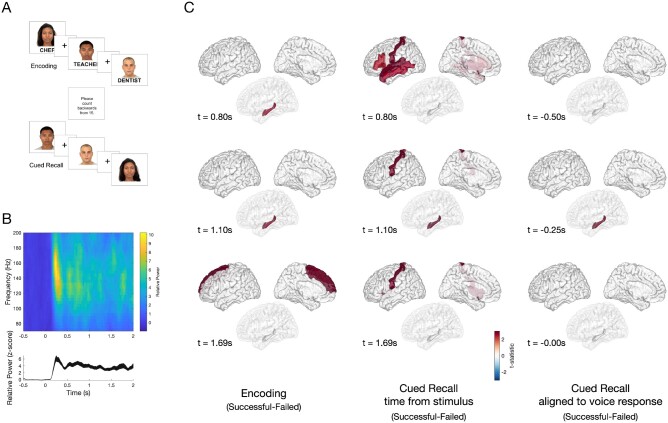
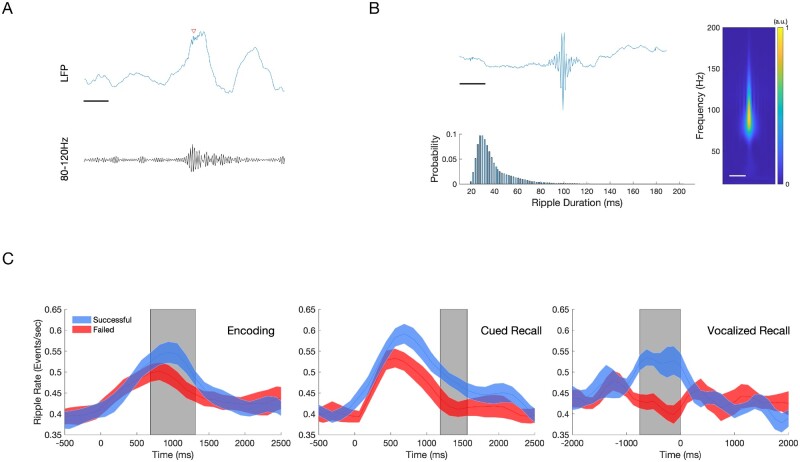
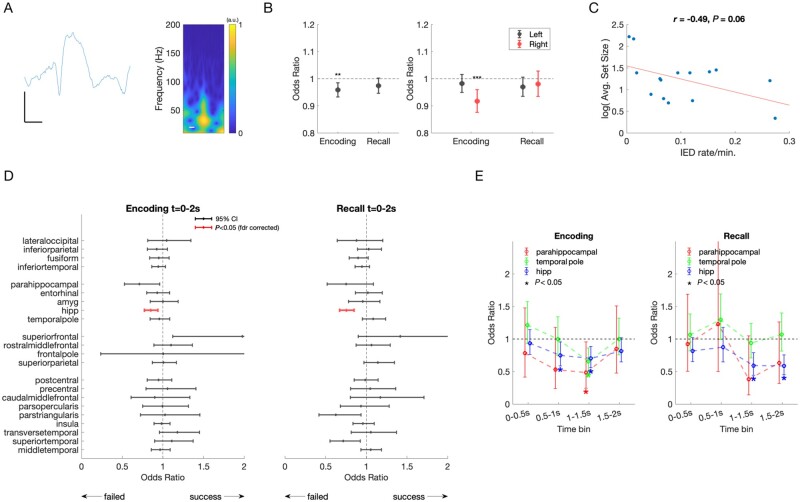
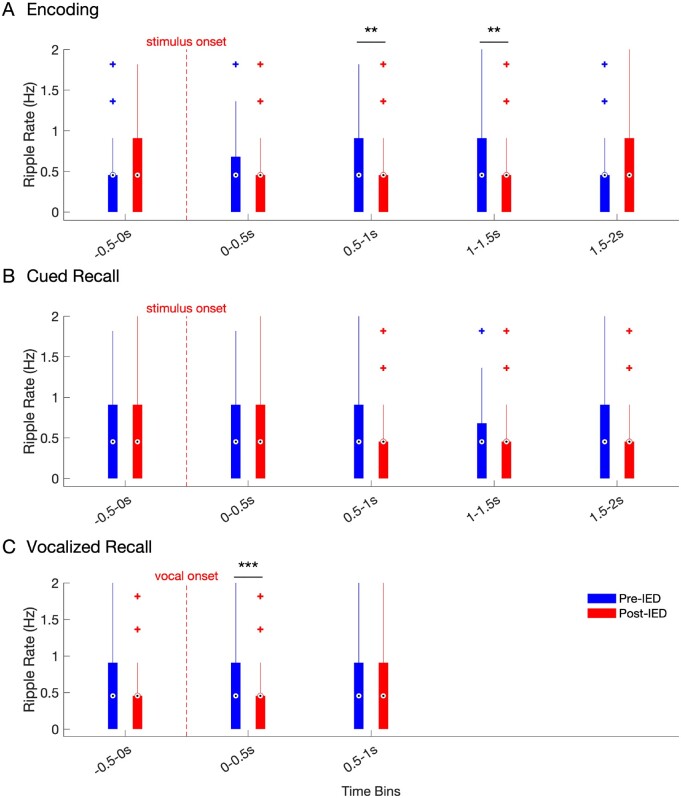
We describe the spatiotemporal course of cortical high-gamma activity, hippocampal ripple activity and interictal epileptiform discharges during an associative memory task in 15 epilepsy patients undergoing invasive EEG. Successful encoding trials manifested significantly greater high-gamma activity in hippocampus and frontal regions. Successful cued recall trials manifested sustained high-gamma activity in hippocampus compared to failed responses. Hippocampal ripple rates were greater during successful encoding and retrieval trials. Interictal epileptiform discharges during encoding were associated with 15% decreased odds of remembering in hippocampus (95% confidence interval 6-23%). Hippocampal interictal epileptiform discharges during retrieval predicted 25% decreased odds of remembering (15-33%). Odds of remembering were reduced by 25-52% if interictal epileptiform discharges occurred during the 500-2000 ms window of encoding or by 41% during retrieval. During encoding and retrieval, hippocampal interictal epileptiform discharges were followed by a transient decrease in ripple rate. We hypothesize that interictal epileptiform discharges impair associative memory in a regionally and temporally specific manner by decreasing physiological hippocampal ripples necessary for effective encoding and recall. Because dynamic memory impairment arises from pathological interictal epileptiform discharge events competing with physiological ripples, interictal epileptiform discharges represent a promising therapeutic target for memory remediation in patients with epilepsy.
Keywords: epilepsy; epileptiform discharges; gamma oscillations; interictal spikes; intracranial EEG.
© The Author(s) (2021). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Fisher RS, Vickrey BG, Gibson P, et al. The impact of epilepsy from the patient's perspective I. Descriptions and subjective perceptions. Epilepsy Res. 2000;41:39-51. - PubMed
-
- Lemesle B, Planton M, Pages B, et al. Accelerated long-term forgetting and autobiographical memory disorders in temporal lobe epilepsy: one entity or two? Rev Neurol (Paris). 2017;173:498-505. - PubMed
-
- Schwab RS. A method of measuring consciousness in attacks of petit mall epilepsy. Arch Neurol Psychiatry. 1939;41:215-217.
-
- Aarts JH, Binnie CD, Smit AM, et al. Selective cognitive impairment during focal and generalized epileptiform EEG activity. Brain. 1984;107:293-308. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
