

Determination of initial airtightness after anatomical laser segmentectomy in an ex vivo model
- PMID: 33891211
- PMCID: PMC8918094
- DOI: 10.1007/s10103-021-03312-2
Determination of initial airtightness after anatomical laser segmentectomy in an ex vivo model
Abstract
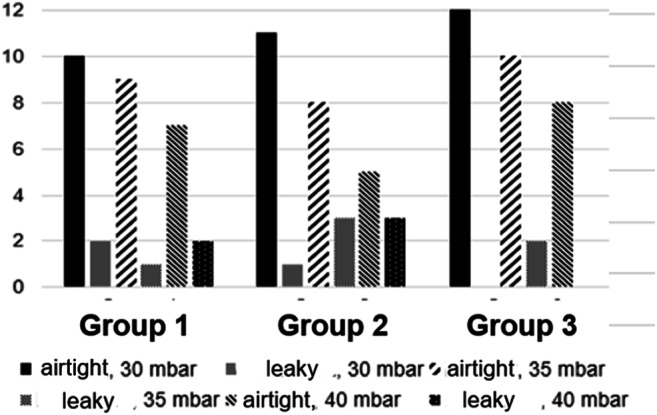
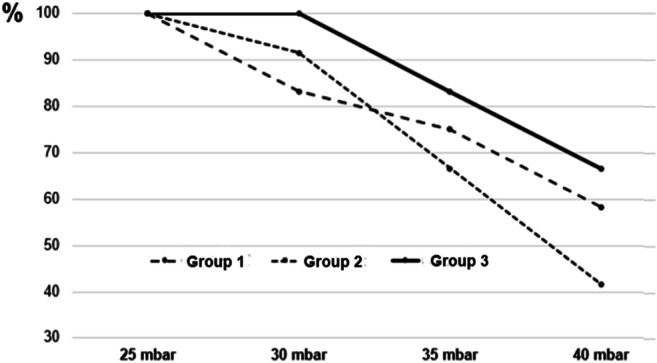
If a pulmonary pathology can be removed by anatomical segmentectomy, the need for lobectomy is obviated. The procedure is considered oncologically equivalent and saves healthy lung tissue. In every segmentectomy, lung parenchyma must be transected in the intersegmental plane. Using an ex vivo model based on porcine lung, three transection techniques (monopolar cutter + suture, stapler, and Nd:YAG laser) are to be compared with respect to their initial airtightness. At an inspiratory ventilation pressure of 25 mbar, all three preparations were airtight. Upon further increase in ventilation pressure up to 40 mbar, the laser group performed best in terms of airtightness. Since thanks to its use of a laser fibre, this technique is particularly suitable for minimally invasive surgery; it should be further evaluated clinically for this indication in the future.
Keywords: Airtightness; Laser fibre; Monopolar cutter; Nd:YAG laser; Segmental resection; Segmentectomy; Stapler; VATS.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Campione A, et al. Comparison between segmentectomy and larger resection of stage IA non-small cell lung carcinoma. J Cardiovasc Surg. 2004;45(1):67–70. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
