

Monitoring PSMA Responses to ADT in Prostate Cancer Patient-Derived Xenograft Mouse Models Using [18F]DCFPyL PET Imaging
- PMID: 33891265
- PMCID: PMC9910584
- DOI: 10.1007/s11307-021-01605-0
Monitoring PSMA Responses to ADT in Prostate Cancer Patient-Derived Xenograft Mouse Models Using [18F]DCFPyL PET Imaging
Abstract
Purpose: PSMA overexpression has been associated with aggressive prostate cancer (PCa). However, PSMA PET imaging has revealed highly variable changes in PSMA expression in response to ADT treatment ranging from increases to moderate decreases. To better understand these PSMA responses and potential relationship to progressive PCa, the PET imaging agent, [18F]DCFPyL, was used to assess changes in PSMA expression in response to ADT using genomically characterized LuCaP patient-derived xenograft mouse models (LuCaP-PDXs) which were found to be sensitive to ADT (LuCaP73 and LuCaP136;CS) or resistant (LuCaP167;CR).
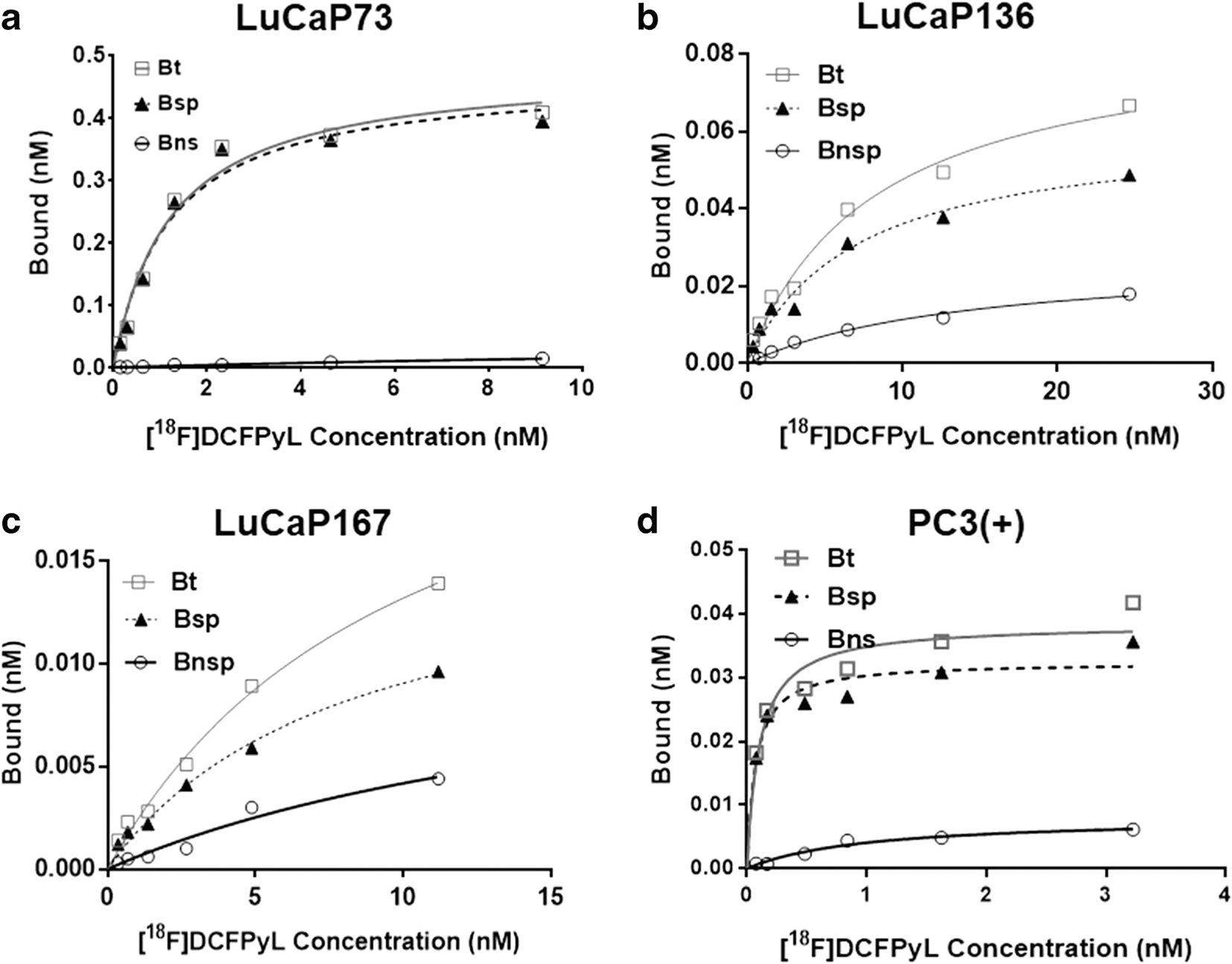
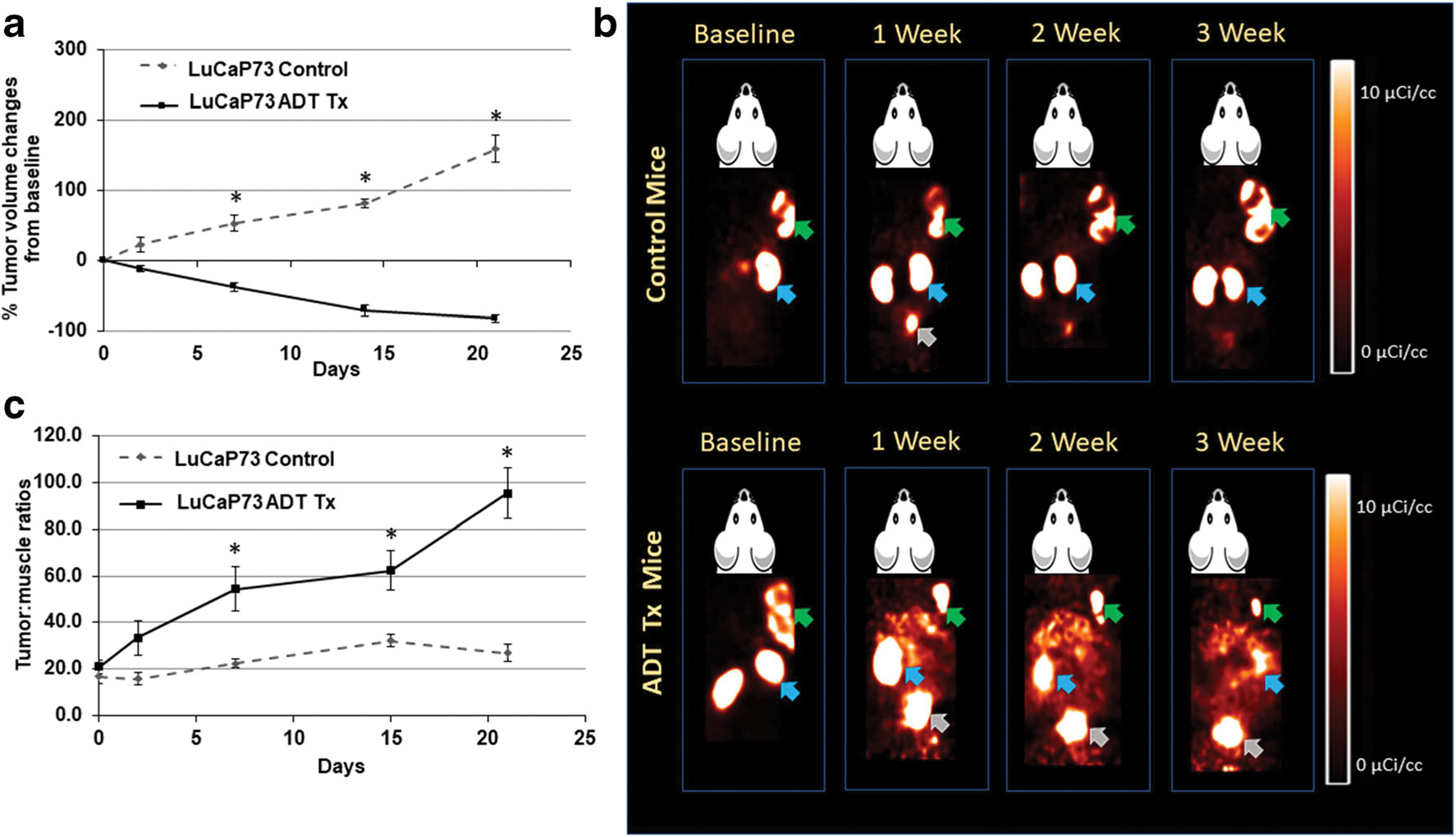
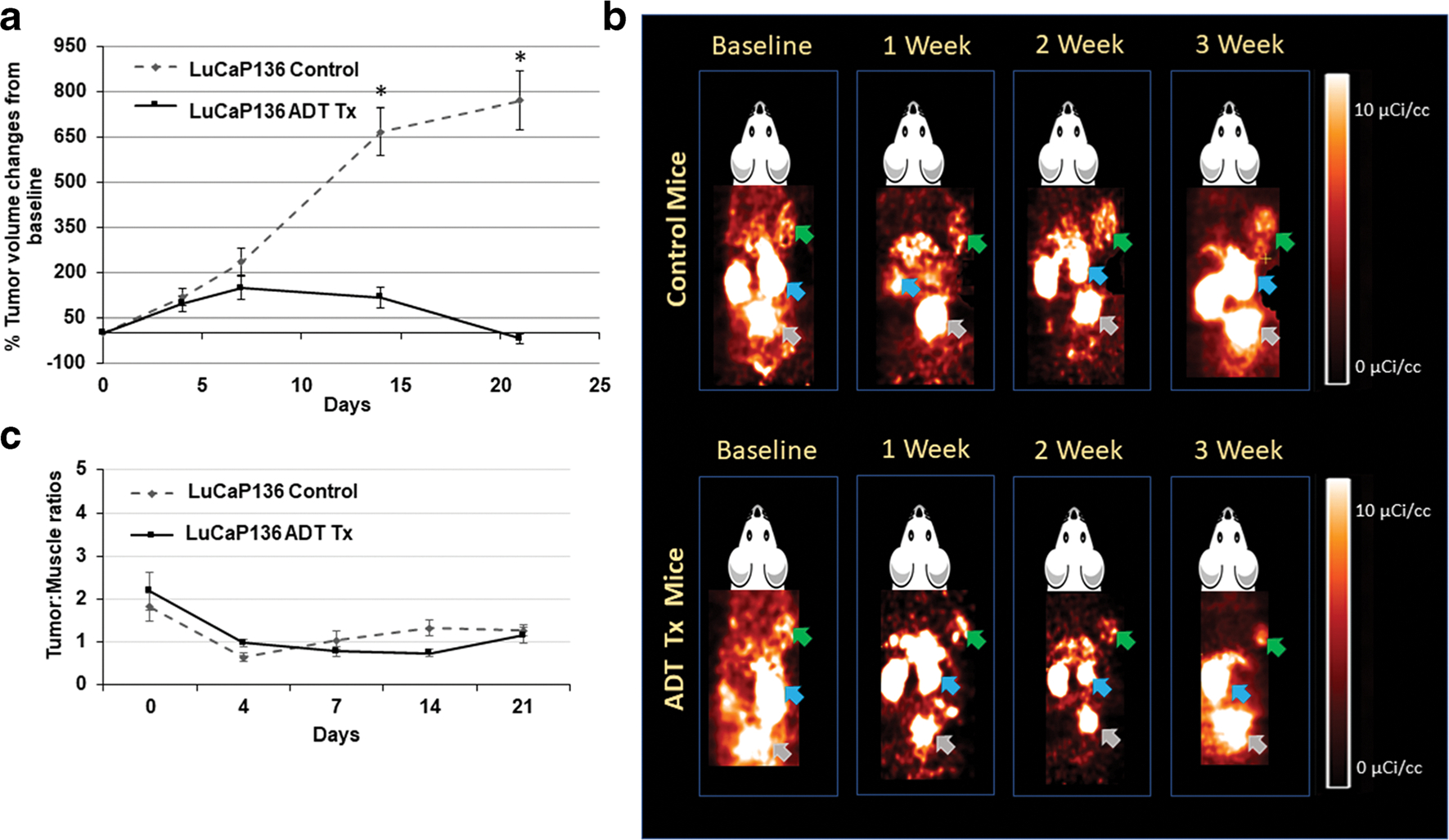
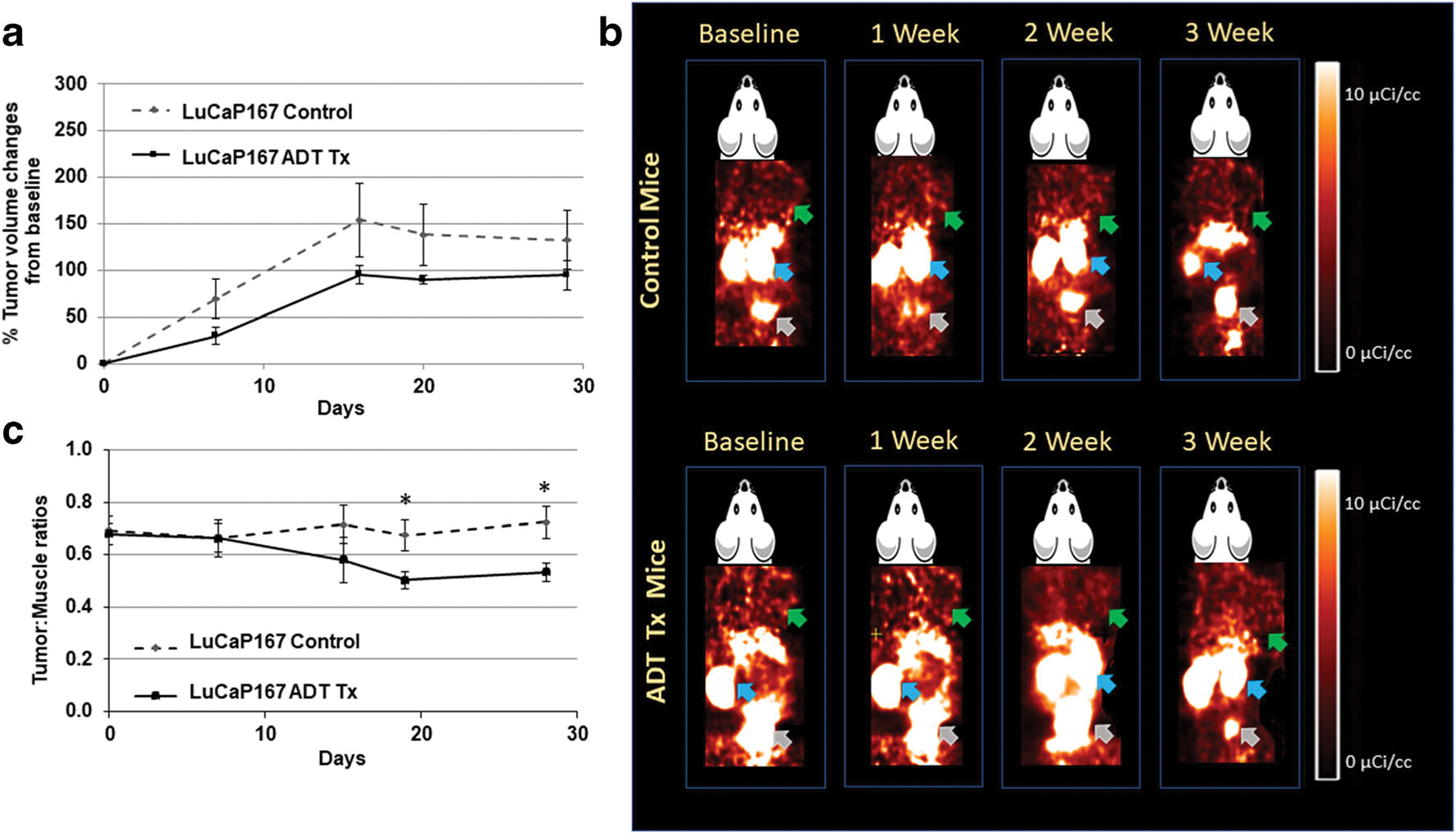
Methods: [18F]DCFPyL (2-(3-{1-carboxy-5-[(6-[18F]fluoro-pyridine-3-carbonyl)-amino]-pentyl}-ureido)-pentanedioic acid) was used to assess PSMA in vitro (saturation assays) in LuCaP tumor membrane homogenates and in vivo (imaging/biodistribution) in LuCaP-PDXs. Control and ADT-treated LuCaPs were imaged before ADT (0 days) and 2-, 7-, 14-, and 21-days post-ADT from which tumor:muscle ratios (T:Ms) were determined and concurrently tumor volumes were measured (caliper). After the 21-day imaging, biodistributions and histologic/genomic (PSMA, AR) analysis were done.
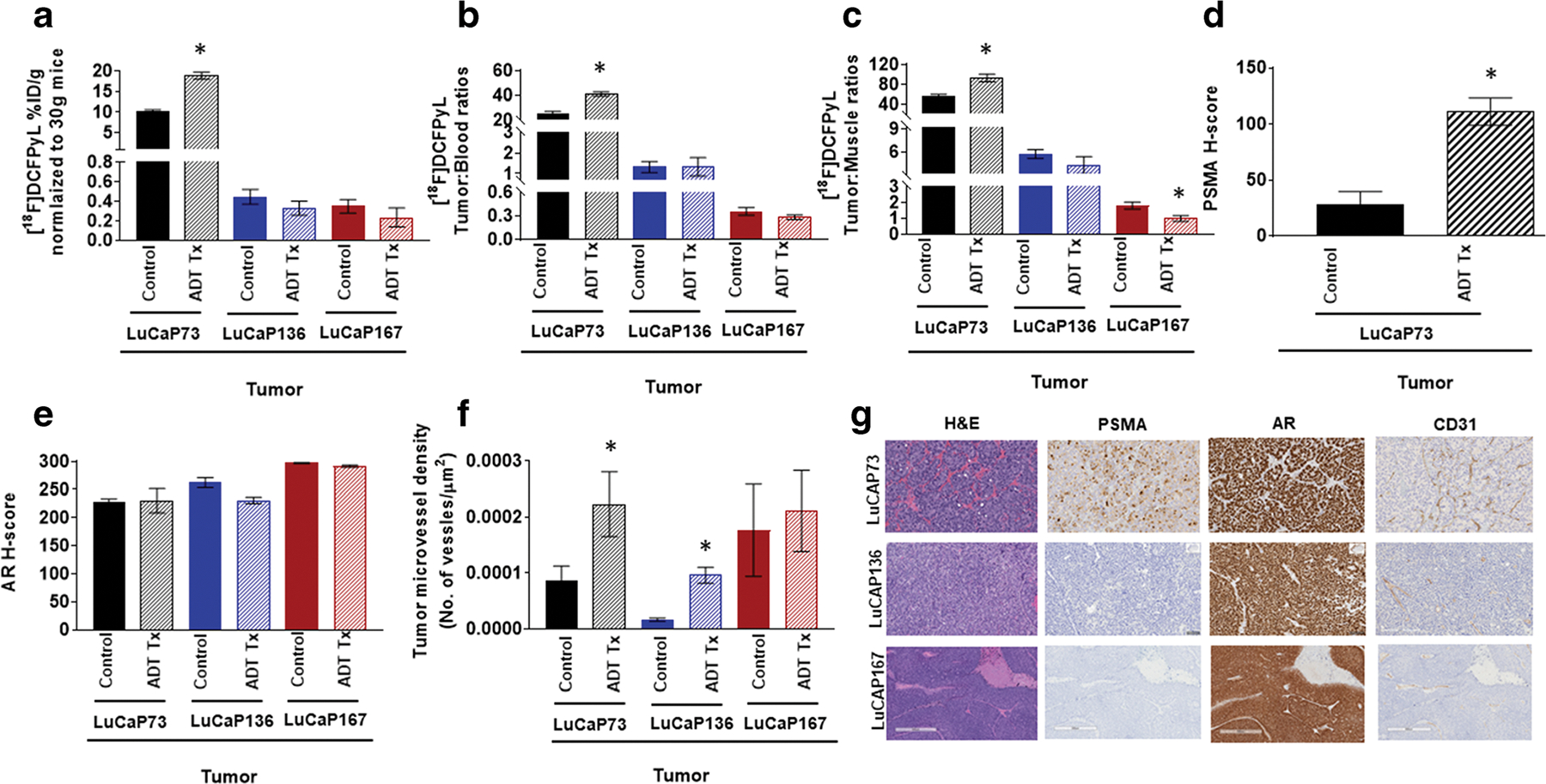
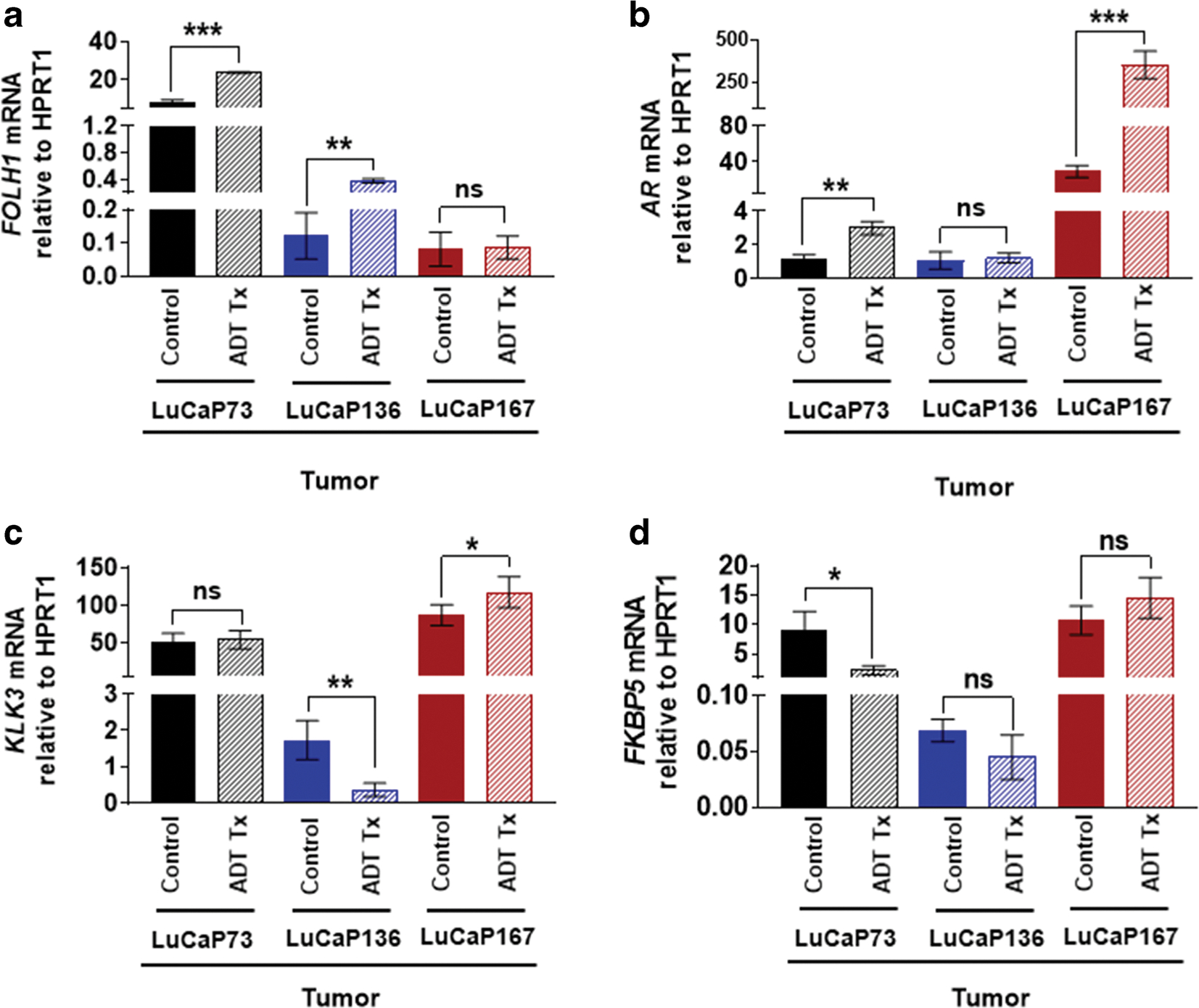
Results: [18F]DCFPyL exhibited high affinity for PSMA and distinguished different levels of PSMA in LuCaP tumors. Post-ADT CS LuCaP73 and LuCaP136 tumor volumes significantly decreased at day 7 or 14 respectively vs controls, whereas the CR LuCaP167 tumor volumes were minimally changed. [18F]DCFPyL imaging T:Ms were increased 3-5-fold in treated LuCaP73 tumors vs controls, while treated LuCaP136 T:Ms remained unchanged which was confirmed by day 21 biodistribution results. For treated LuCaP167, T:Ms were decreased (~ 45 %) vs controls but due to low T:M values (<2) may not be indicative of PSMA level changes. LuCaP73 tumor PSMA histologic/genomic results were comparable to imaging/biodistribution results, whereas the results for other tumor types varied.
Conclusion: Tumor responses to ADT varied from sensitive to resistant among these LuCaP PDXs, while only the high PSMA expressing LuCaP model exhibited an increase in PSMA levels in response to ADT. These models may be useful in understanding the clinical relevance of PSMA PET responses to ADT and potentially the relationship to disease progression as it may relate to the genomic signature.
Keywords: ADT therapy; Androgen deprivation therapy; LuCaP; PDX; PET imaging; PSMA; Prostate cancer.
© 2021. This is a U.S. government work and not under copyright protection in the U.S.; foreign copyright protection may apply.
Conflict of interest statement
Conflict of Interest
The authors declare that they have no conflict of interest.
Figures
References
-
- Ghosh A, Heston WD (2004) Tumor target prostate specific membrane antigen (PSMA) and its regulation in prostate cancer. J Cell Biochem 91:528–539 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
