

Obesity in Prader-Willi syndrome: physiopathological mechanisms, nutritional and pharmacological approaches
- PMID: 33891302
- PMCID: PMC8421305
- DOI: 10.1007/s40618-021-01574-9
Obesity in Prader-Willi syndrome: physiopathological mechanisms, nutritional and pharmacological approaches
Abstract
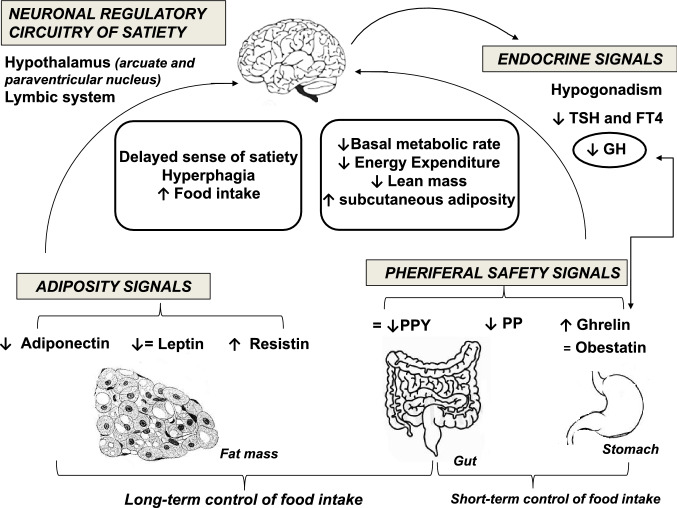
Prader-Willi syndrome (PWS) is a genetic disorder caused by the lack of expression of genes on the paternally inherited chromosome 15q11.2-q13 region. The three main genetic subtypes are represented by paternal 15q11-q13 deletion, maternal uniparental disomy 15, and imprinting defect. Clinical picture of PWS changes across life stages. The main clinical characteristics are represented by short stature, developmental delay, cognitive disability and behavioral diseases. Hypotonia and poor suck resulting in failure to thrive are typical of infancy. As the subjects with PWS age, clinical manifestations such as hyperphagia, temperature instability, high pain threshold, hypersomnia and multiple endocrine abnormalities including growth hormone and thyroid-stimulating hormone deficiencies, hypogonadism and central adrenal insufficiency due to hypothalamic dysfunction occur. Obesity and its complications are the most common causes of morbidity and mortality in PWS. Several mechanisms for the aetiology of obesity in PWS have been hypothesized, which include aberration in hypothalamic pathways of satiety control resulting in hyperphagia, disruption in hormones regulating appetite and satiety and reduced energy expenditure. However, despite the advancement in the research field of the genetic basis of obesity in PWS, there are contradictory data on the management. Although it is mandatory to adopt obesity strategy prevention from infancy, there is promising evidence regarding the management of obesity in adulthood with current obesity drugs along with lifestyle interventions, although the data are limited. Therefore, the current manuscript provides a review of the current evidence on obesity and PWS, covering physiopathological aspects, obesity-related complications and conservative management.
Keywords: Diabetes mellitus; Hyperphagia; Obesity; Prader–Willi syndrome.
© 2021. The Author(s).
Conflict of interest statement
All authors declare no conflict of interests.
Figures
References
-
- Allas S, Caixas A, Poitou C, Coupaye M, Thuilleaux D, Lorenzini F, Diene G, Crino A, Illouz F, Grugni G, et al. AZP-531, an unacylated ghrelin analog, improves food-related behavior in patients with Prader–Willi syndrome: a randomized placebo-controlled trial. PLoS ONE. 2018;13:e0190849. doi: 10.1371/journal.pone.0190849. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
