

Clinical Audit of Survival Outcomes and Prognostic Factors in Adolescents and Adults with Medulloblastoma
- PMID: 33891492
- PMCID: PMC8864430
- DOI: 10.1089/jayao.2021.0034
Clinical Audit of Survival Outcomes and Prognostic Factors in Adolescents and Adults with Medulloblastoma
Abstract
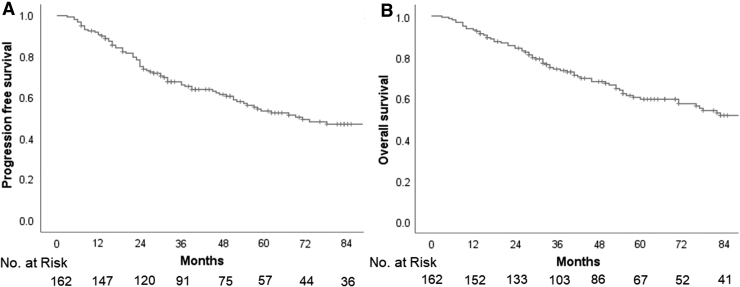
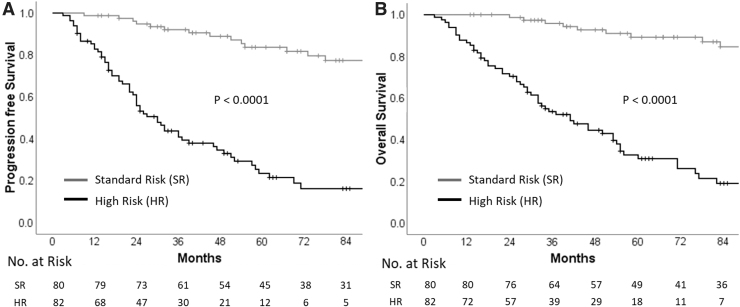
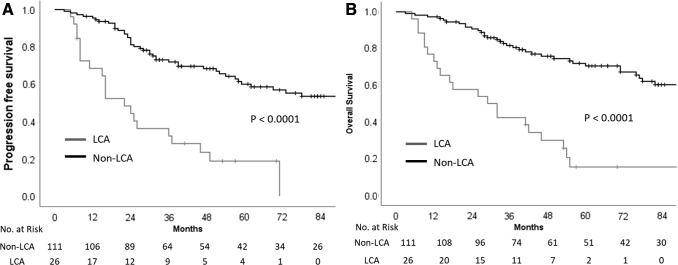
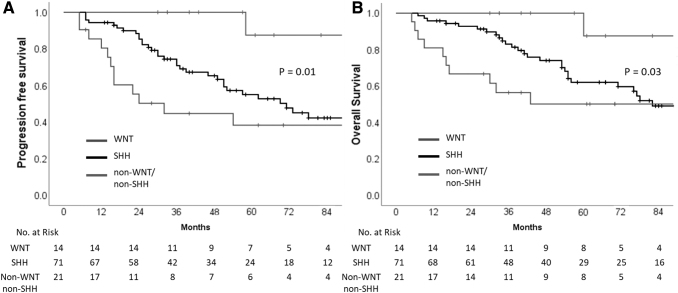
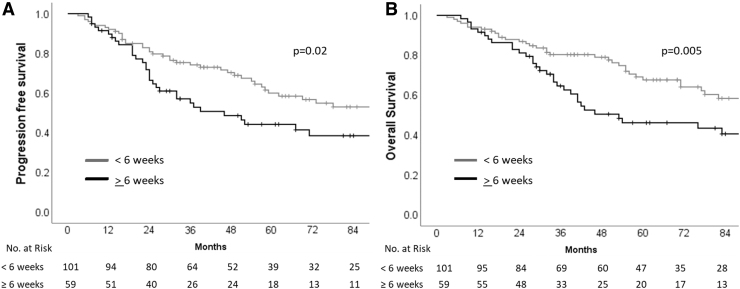
Purpose: Medulloblastomas, comprising 20%-25% of all primary brain tumors in children are much rarer in adulthood. Disease biology varies substantially across different age groups; however, owing to rarity, adults with medulloblastoma are traditionally treated using pediatric protocols. This is a retrospective audit of adolescent and adult medulloblastoma from a comprehensive cancer center. Methods: Data regarding demography, clinical presentation, imaging characteristics, histopathological features, molecular profiling, risk stratification, treatment details, and outcomes were retrieved from medical records. All time-to-event outcomes were analyzed using Kaplan-Meier method and compared with the log-rank test. Univariate and multivariate analysis of relevant prognostic factors was done with p value <0.05 being considered statistically significant. Results: A total of 162 patients ≥15 years of age with medulloblastoma were included. The median age was 25 years (range: 15-59 years) with leptomeningeal metastases seen in 31 (19%) patients at initial diagnosis. Following surgery, patients were treated with appropriate risk-stratified adjuvant therapy comprising of craniospinal irradiation plus boost with or without systemic chemotherapy. At a median follow-up of 50 months, 5-year Kaplan-Meier estimates of progression-free survival and overall survival were 53.5% and 59.5%, respectively. The addition of adjuvant systemic chemotherapy did not impact upon survival in standard-risk medulloblastoma. High-risk (HR) disease and anaplastic histology emerged as significant and independent predictors of poor survival on multivariate analysis. Conclusion: Medulloblastoma is a rare tumor in adolescents and adults with key differences in disease biology and resultant outcomes compared with the pediatric population. Contemporary management comprising maximal safe resection followed by appropriate risk-stratified adjuvant therapy provides acceptable survival outcomes.
Keywords: biology; medulloblastoma; outcomes; risk-stratification.
Conflict of interest statement
None of the authors has any conflict of interest to declare.
Figures
References
-
- Majd N, Penas-Prado M. Updates on management of adult medulloblastoma. Curr Treat Options Oncol. 2019;20:64. - PubMed
-
- Vadgaonkar R, Epari S, Chinnaswamy G, et al. . Distinct demographic profile and molecular markers of primary CNS tumor in 1873 adolescent and young adult patient population. Childs Nerv Syst. 2018;34:1489–95. - PubMed
-
- Zeltzer PM, Boyett JM, Finlay JL, et al. . Metastasis stage, adjuvant treatment, and residual tumor are prognostic factors for medulloblastoma in children: conclusions from the Children's Cancer Group 921 randomized phase III study. J Clin Oncol. 1999;17:832–45. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
