

doi: 10.1371/journal.pmed.1003561.
eCollection 2021 Apr.
The prevention and treatment of Plasmodium vivax malaria
Affiliations
- PMID: 33891587
- PMCID: PMC8064578
- DOI: 10.1371/journal.pmed.1003561
Item in Clipboard
The prevention and treatment of Plasmodium vivax malaria
PLoS Med.
.
Abstract
Cindy S Chu and co-authors review options for diagnosis, safe and radical cure, and relapse prevention of Plasmodium Vivax.
Conflict of interest statement
We have read the journal’s policy and the authors of this manuscript have the following competing interests: NJW is an Academic Editor on PLOS Medicine’s editorial board.
Figures
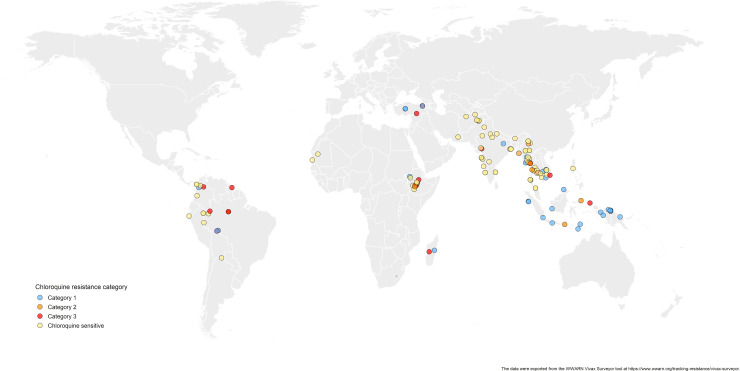
The data were exported from the WWARN Vivax Surveyor tool at https://www.wwarn.org/tracking-resistance/vivax-surveyor . Evidence for chloroquine resistance comes from P. vivax clinical trials published from 1985–2019. Some trials are from different years in the same area; this figure does not specify the change in chloroquine resistance pattern over time. CQS: Chloroquine sensitive, Category 1: very suggestive of resistance, Category 2: suggestive of resistance, Category 3: potential evidence of resistance.
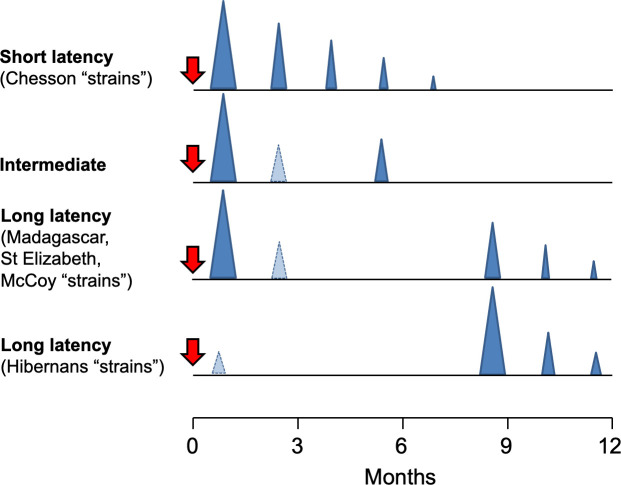
The temporal patterns of P. vivax relapse in different “strains.” The red arrow indicates the infective mosquito bite which leads to the primary infection. The blue triangles represent patent P. vivax infections; the largest triangle is the primary infection. The proportions of successive relapses decline, and there is an increasing probability that the relapses are oligosymptomatic or asymptomatic. The translucent blue triangles are P. vivax infections which may sometimes occur. The short latency frequent relapse pattern (typified by the “Chesson strain”) is prevalent across tropical areas. The intermediate phenotype may occur in South Asia. The long latency phenotype (typified by the Madagascar, St Elizabeth, and McCoy strains) is found in Central America, North Africa, and central Asia, while the long latency “hibernans” phenotype, which was prevalent in Northern Europe and Russia, is still found in North Korea.
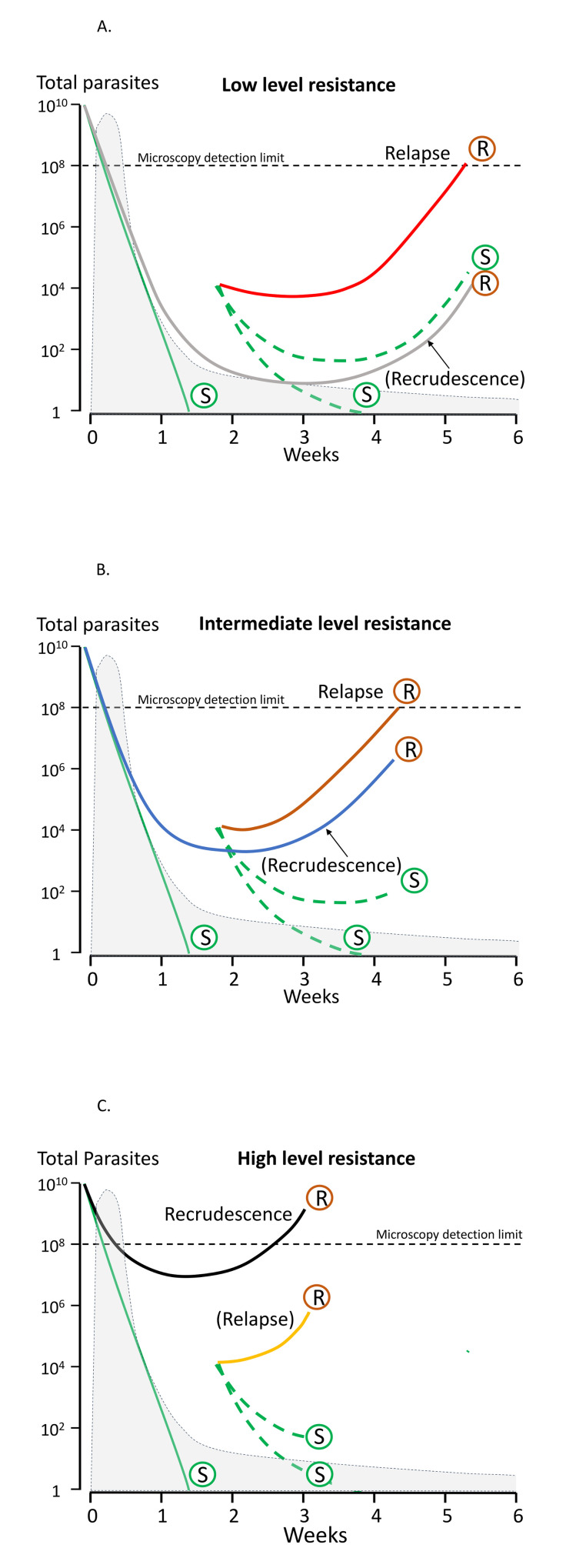
The vertical axis shows the total number of parasites in the body in acute vivax malaria. The light grey shaded area is the blood chloroquine concentration profile. The limit of microscopy detection is approximately 50 parasites/uL. In each panel, chloroquine-sensitive parasites are shown by green lines and marked S. The relapses emerge from the liver approximately 2 weeks after starting treatment. There is uncertainty whether chloroquine eliminates or temporarily suppresses the first relapse (in most cases it suppresses but does not eliminate [118]) so dotted lines representing both scenarios are shown. Resistant parasites causing relapse and recrudescence are marked R. Upper panel (A): When there are low levels of resistance, the blood stage infection is cleared usually by the schizonticide, and the first relapse is suppressed until the drug levels fall below the mean inhibitory concentration (MIC) (e.g., in this illustrated example, chloroquine levels above the MIC are maintained until day 28, and relapse parasitaemia becomes patent 2 weeks later) [125]. Recrudescence is very unlikely (occurring only in those patients with low drug levels) and in patients with relapse, the recrudescence would not be detected because the relapse appears first. Middle panel (B): When resistance to chloroquine is at an intermediate level, the blood stage infection clears, but the first relapse becomes patent before 28 days. If a relapse occurs, it would still preempt any recrudescence. Lower panel (C): With high levels of resistance, the blood stage infection recrudesces before the relapse parasitaemia becomes patent.
References
-
- World Health Organization. World malaria Report 2020. Geneva; 2020. Available from: https://www.who.int/publications/i/item/9789240015791
MeSH terms
LinkOut - more resources
Full Text Sources
