

Risk factors for surgery-related muscle quantity and muscle quality loss and their impact on outcome
- PMID: 33892809
- PMCID: PMC8063361
- DOI: 10.1186/s40001-021-00507-9
Risk factors for surgery-related muscle quantity and muscle quality loss and their impact on outcome
Abstract
Background: Surgery-related loss of muscle quantity negatively affects postoperative outcomes. However, changes of muscle quality have not been fully investigated. A perioperative intervention targeting identified risk factors could improve postoperative outcome. This study investigated risk factors for surgery-related loss of muscle quantity and quality and outcomes after liver resection for colorectal liver metastasis (CRLM).
Methods: Data of patients diagnosed with CRLM who underwent liver resection between 2006 and 2016 were analysed. Muscle quantity (psoas muscle index [PMI]), and muscle quality, (average muscle radiation attenuation [AMA] of the psoas), were measured using computed tomography. Changes in PMI and AMA of psoas after surgery were assessed.
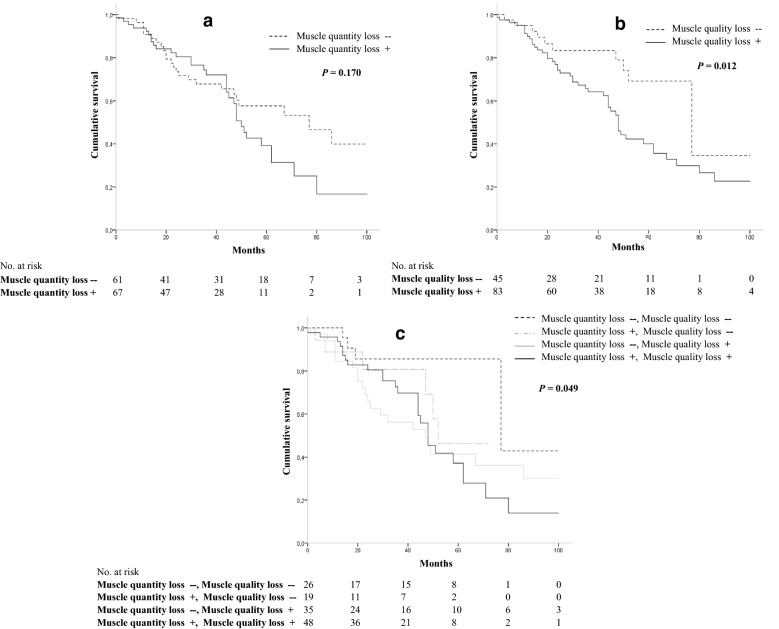
Results: A total of 128 patients were analysed; 67 (52%) had surgery-related loss of muscle quantity and 83 (65%) muscle quality loss. Chronic obstructive pulmonary disease (COPD) (P = 0.045) and diabetes (P = 0.003) were risk factors for surgery-related loss of muscle quantity. A higher age (P = 0.002), open resection (P = 0.003) and longer operation time (P = 0.033) were associated with muscle quality loss. Overall survival was lower in patients with both muscle quantity and quality loss compared to other categories (P = 0.049). The rate of postoperative complications was significantly higher in the group with surgery-related loss of muscle quality.
Conclusions: Risk factors for surgery-related muscle loss were identified. Overall survival was lowest in patients with both muscle quantity and quality loss. Complication rate was higher in patients with surgery-related loss of muscle quality.
Keywords: Colorectal liver metastasis; Liver resection; Psoas muscle index; Surgery-related muscle quality loss; Surgery-related muscle quantity loss; Total psoas area.
Conflict of interest statement
The authors declare no competing interests
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
