

Deep learning to detect acute respiratory distress syndrome on chest radiographs: a retrospective study with external validation
- PMID: 33893070
- PMCID: PMC8182690
- DOI: 10.1016/S2589-7500(21)00056-X
Deep learning to detect acute respiratory distress syndrome on chest radiographs: a retrospective study with external validation
Abstract
Background: Acute respiratory distress syndrome (ARDS) is a common, but under-recognised, critical illness syndrome associated with high mortality. An important factor in its under-recognition is the variability in chest radiograph interpretation for ARDS. We sought to train a deep convolutional neural network (CNN) to detect ARDS findings on chest radiographs.
Methods: CNNs were pretrained on 595 506 radiographs from two centres to identify common chest findings (eg, opacity and effusion), and then trained on 8072 radiographs annotated for ARDS by multiple physicians using various transfer learning approaches. The best performing CNN was tested on chest radiographs in an internal and external cohort, including a subset reviewed by six physicians, including a chest radiologist and physicians trained in intensive care medicine. Chest radiograph data were acquired from four US hospitals.
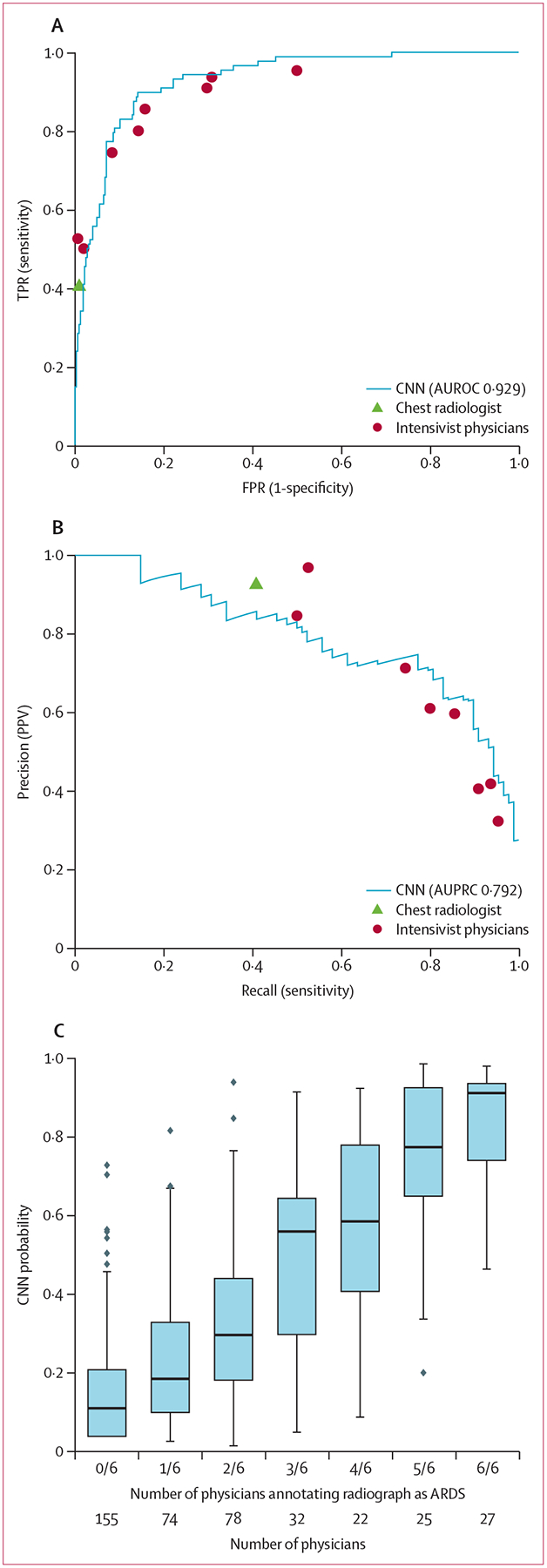
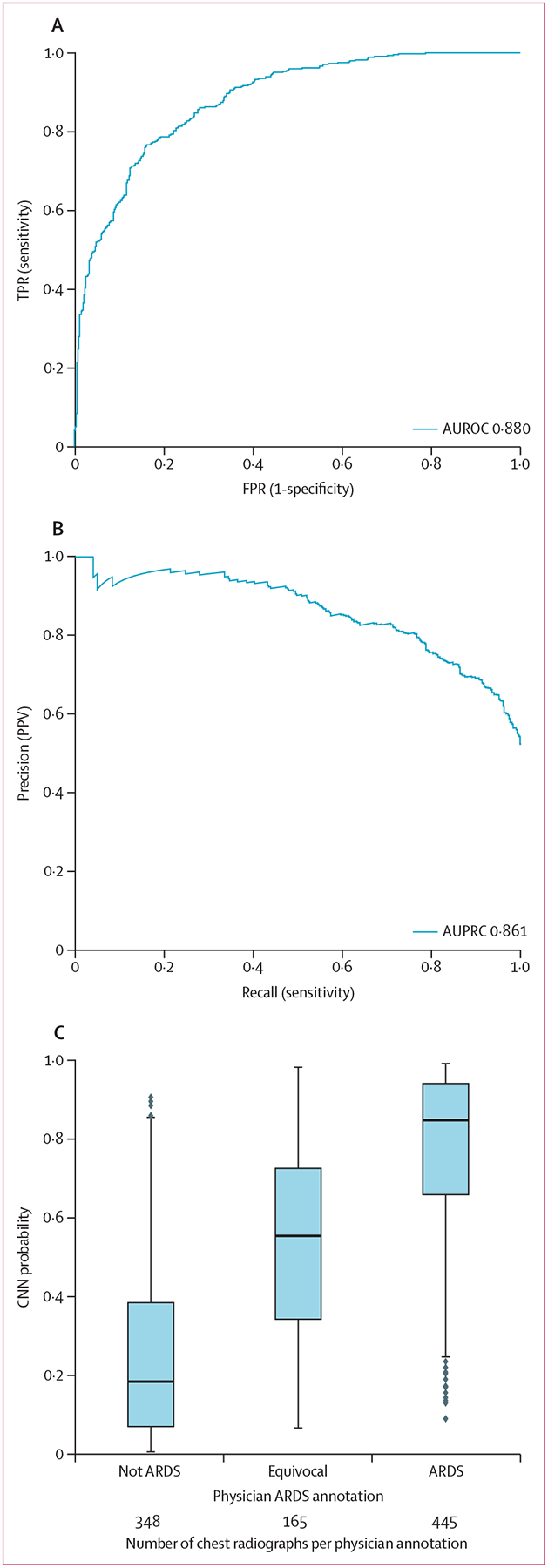
Findings: In an internal test set of 1560 chest radiographs from 455 patients with acute hypoxaemic respiratory failure, a CNN could detect ARDS with an area under the receiver operator characteristics curve (AUROC) of 0·92 (95% CI 0·89-0·94). In the subgroup of 413 images reviewed by at least six physicians, its AUROC was 0·93 (95% CI 0·88-0·96), sensitivity 83·0% (95% CI 74·0-91·1), and specificity 88·3% (95% CI 83·1-92·8). Among images with zero of six ARDS annotations (n=155), the median CNN probability was 11%, with six (4%) assigned a probability above 50%. Among images with six of six ARDS annotations (n=27), the median CNN probability was 91%, with two (7%) assigned a probability below 50%. In an external cohort of 958 chest radiographs from 431 patients with sepsis, the AUROC was 0·88 (95% CI 0·85-0·91). When radiographs annotated as equivocal were excluded, the AUROC was 0·93 (0·92-0·95).
Interpretation: A CNN can be trained to achieve expert physician-level performance in ARDS detection on chest radiographs. Further research is needed to evaluate the use of these algorithms to support real-time identification of ARDS patients to ensure fidelity with evidence-based care or to support ongoing ARDS research.
Funding: National Institutes of Health, Department of Defense, and Department of Veterans Affairs.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests The University of Michigan has filed a US Utility Patent application (number 17/082,145) for the invention, University of Michigan IR number 2020–026, Computer vision technologies for rapid disease detection, which uses software technology to process chest radiographs to detect acute diseases, of which MWS, DT, CEG, and KRW report being coinventors, which is related to work reported in this Article. NJM reports fees paid to her institution by Quantum Leap. Healthcare Consortium, Biomark, Athersys, and The Marcus Foundation for work unrelated to the current Article. All other authors declare no competing interests.
Figures
References
-
- Fan E, Del Sorbo L, Goligher EC, et al. An official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine clinical practice guideline: mechanical ventilation in adult patients with acute respiratory distress syndrome. Am J Respir Crit Care Med 2017; 195: 1253–63. - PubMed
-
- Bellani G, Laffey JG, Pham T, et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA 2016; 315: 788–800. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
