

Automated, multiparametric monitoring of respiratory biomarkers and vital signs in clinical and home settings for COVID-19 patients
- PMID: 33893178
- PMCID: PMC8126790
- DOI: 10.1073/pnas.2026610118
Automated, multiparametric monitoring of respiratory biomarkers and vital signs in clinical and home settings for COVID-19 patients
Abstract
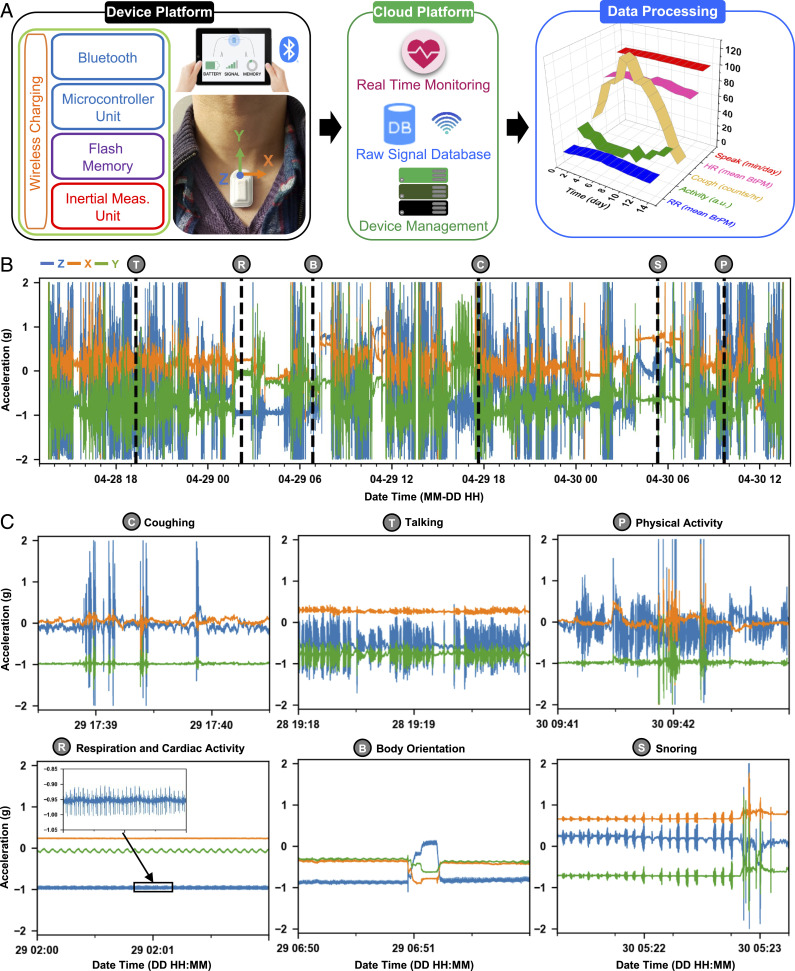
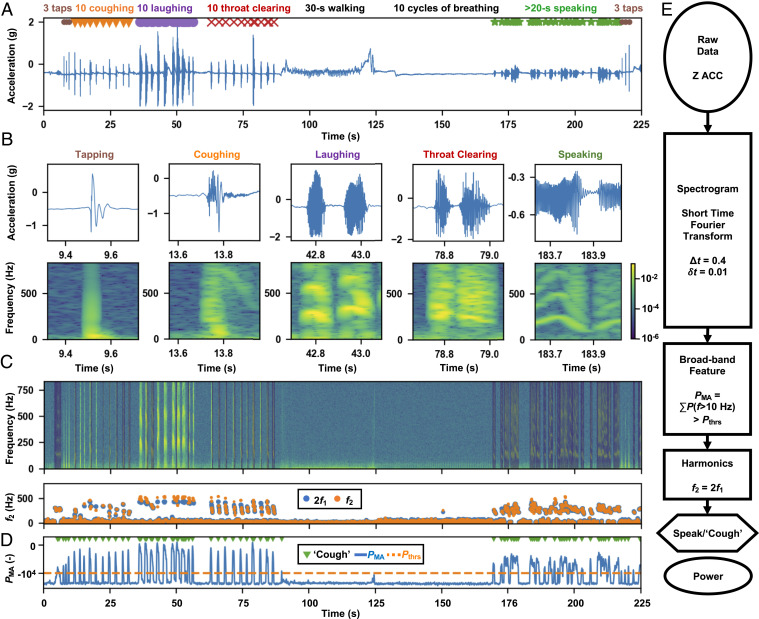
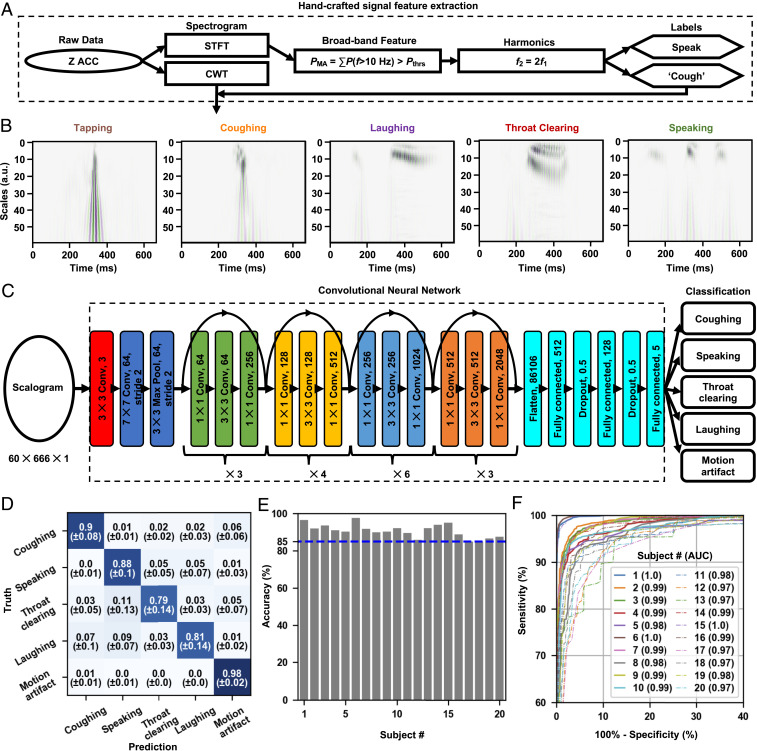
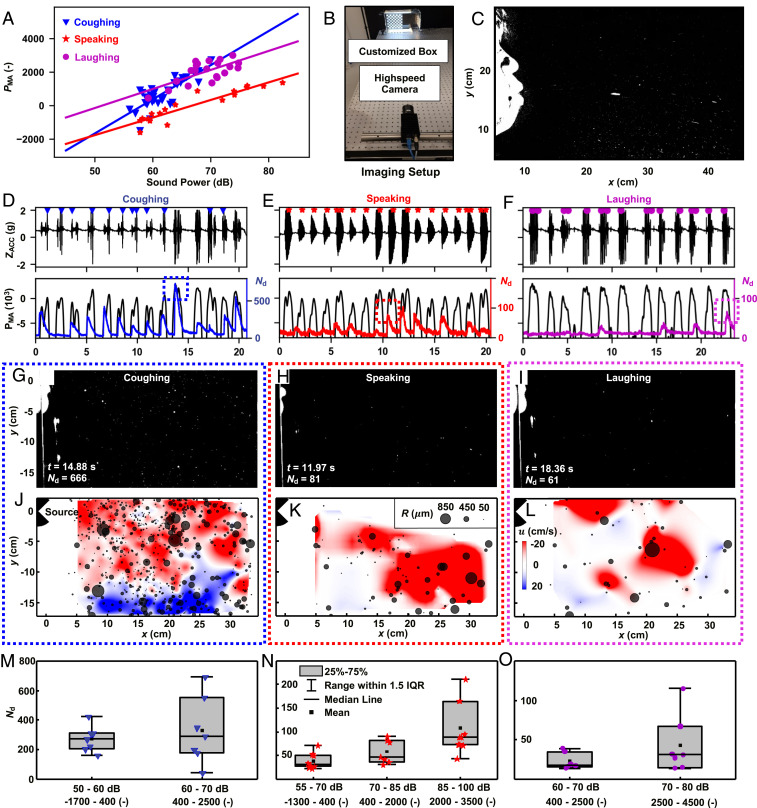
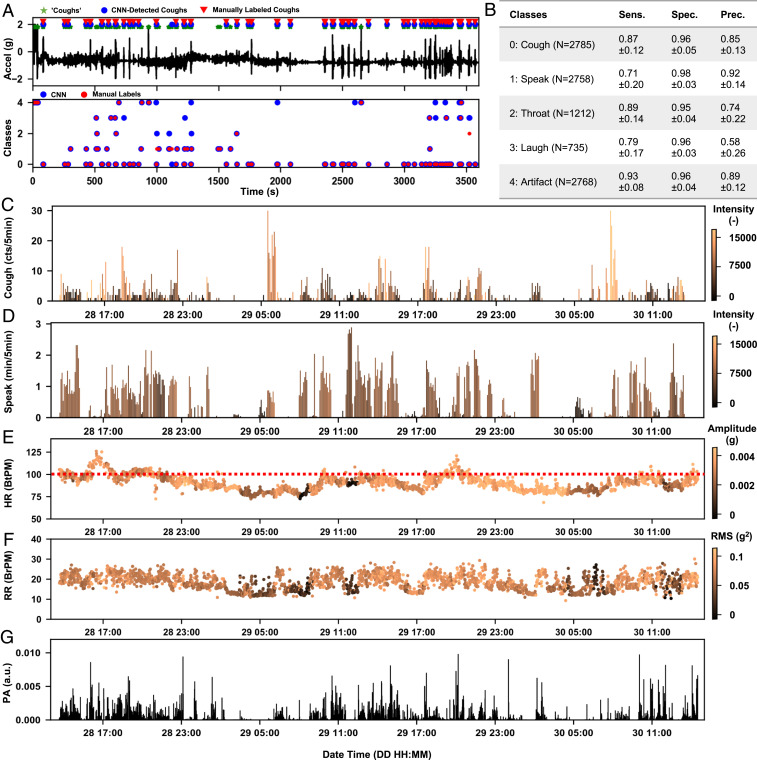
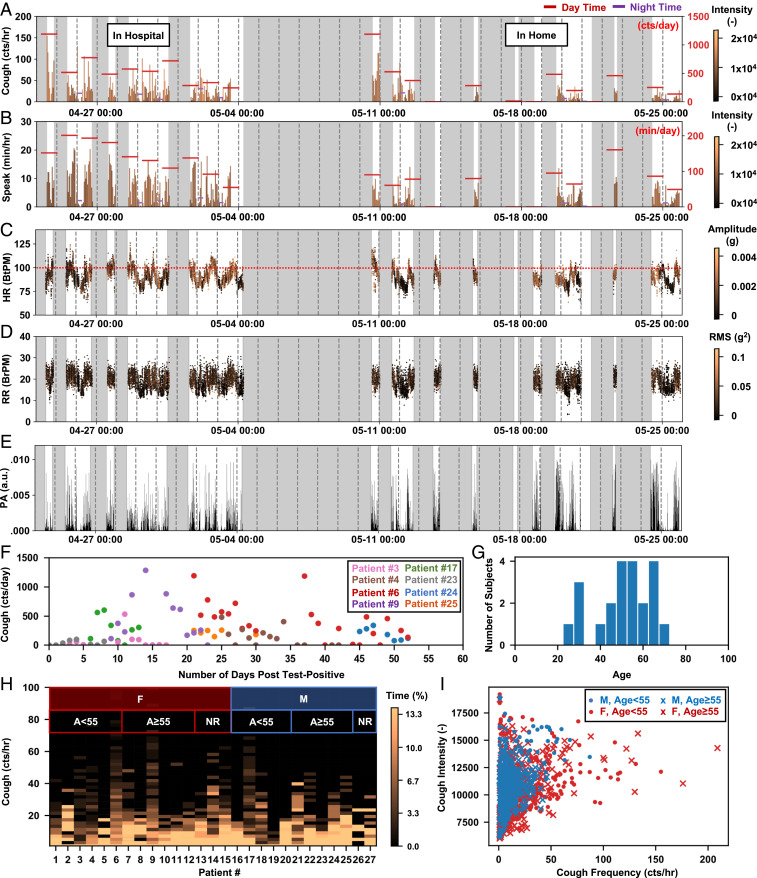
Capabilities in continuous monitoring of key physiological parameters of disease have never been more important than in the context of the global COVID-19 pandemic. Soft, skin-mounted electronics that incorporate high-bandwidth, miniaturized motion sensors enable digital, wireless measurements of mechanoacoustic (MA) signatures of both core vital signs (heart rate, respiratory rate, and temperature) and underexplored biomarkers (coughing count) with high fidelity and immunity to ambient noises. This paper summarizes an effort that integrates such MA sensors with a cloud data infrastructure and a set of analytics approaches based on digital filtering and convolutional neural networks for monitoring of COVID-19 infections in sick and healthy individuals in the hospital and the home. Unique features are in quantitative measurements of coughing and other vocal events, as indicators of both disease and infectiousness. Systematic imaging studies demonstrate correlations between the time and intensity of coughing, speaking, and laughing and the total droplet production, as an approximate indicator of the probability for disease spread. The sensors, deployed on COVID-19 patients along with healthy controls in both inpatient and home settings, record coughing frequency and intensity continuously, along with a collection of other biometrics. The results indicate a decaying trend of coughing frequency and intensity through the course of disease recovery, but with wide variations across patient populations. The methodology creates opportunities to study patterns in biometrics across individuals and among different demographic groups.
Keywords: COVID-19; biomarkers; digital health; respiratory disease; wearable electronics.
Copyright © 2021 the Author(s). Published by PNAS.
Conflict of interest statement
Competing interest statement: X.N., H.J., J.Y.L., K.L., A.J., S.X., and J.A.R. report inventorships and potential royalties in patents assigned to Northwestern University. M.K. and J.Y.L. are employees of a small private company with a commercial interest in the technology. A.R.B., S.X., and J.A.R. report equity ownership in a small private company with a commercial interest in the technology.
Figures
References
-
- Centers for Disease Control and Prevention , Coronavirus disease 2019 (COVID-19). Cases in the U.S. New cases by day. https://covid.cdc.gov/covid-data-tracker/. Accessed 26 December 2020.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
