

Predictors of early recurrence following neoadjuvant chemotherapy and surgical resection for localized pancreatic adenocarcinoma
- PMID: 33893740
- PMCID: PMC8653430
- DOI: 10.1002/jso.26510
Predictors of early recurrence following neoadjuvant chemotherapy and surgical resection for localized pancreatic adenocarcinoma
Abstract
Background and objectives: Neoadjuvant chemotherapy (NAT) for pancreatic adenocarcinoma (PDAC) is increasingly being utilized. However, a significant number of patients will experience early recurrence, possibly negating the benefit of surgery. We aimed to identify factors implicated in early disease recurrence.
Methods: A retrospective review of pancreaticoduodenectomies performed between 2005 and 2017 at our institution for PDAC following NAT was performed. A 6-month cut-off was used to stratify patients into early/late recurrence groups. Multivariate analysis was performed to identify predictors of recurrence.
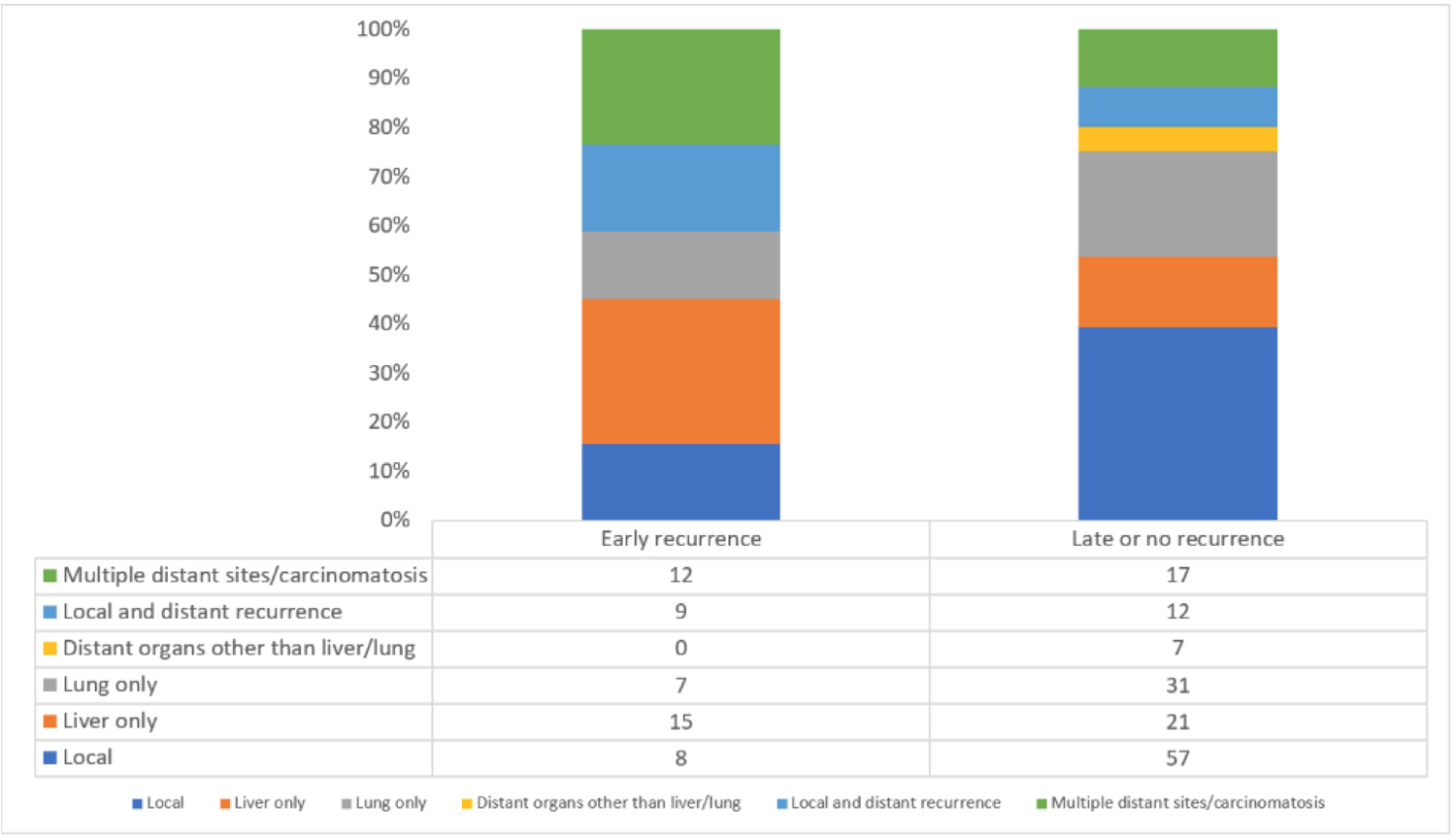
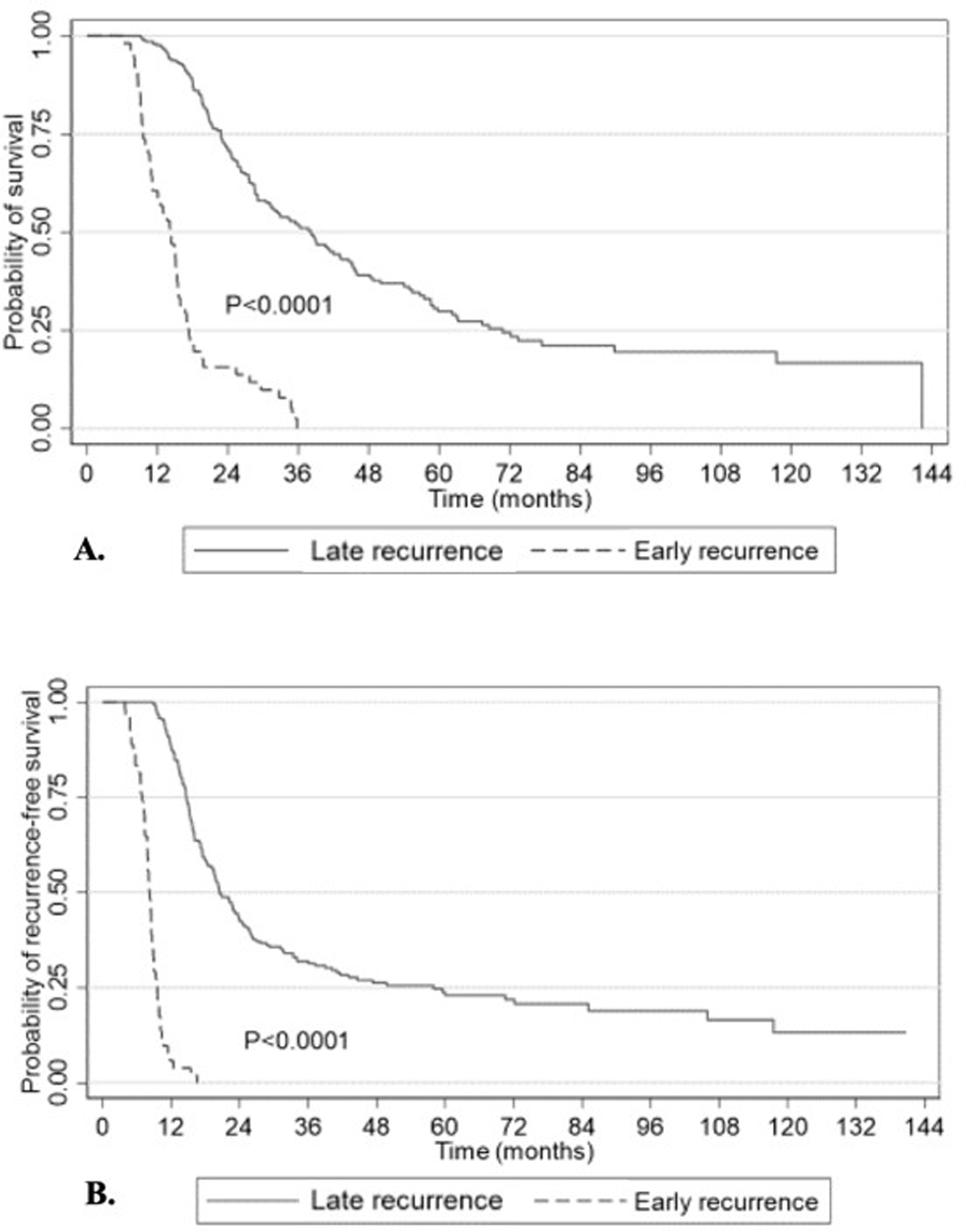
Results: Of 273 patients, 64 (23%) developed early recurrence or died within 90 days of surgery. The median time to recurrence was 4 months (95% confidence interval [CI]: 2.2-4.3) in the early group versus 16 months (95% CI: 13.7-19.9) in the late group. The former had higher baseline and post-NAT Ca19-9 levels than the latter (472 vs. 153 IU/ml, p = 0.001 and 71 vs. 39 IU/ml, p = 0.005, respectively). A higher positive lymph node ratio significantly increased the risk of early recurrence (hazard ratio [HR]: 15.9, p < 0.001) while adjuvant chemotherapy was protective (HR: 0.4, p < 0.001).
Conclusion: Our findings acknowledge the limitations of clinically measured factors used to ascertain response to NAT and underline the need for individualized molecular markers that take into consideration the specific tumor biology.
Keywords: early recurrence; neoadjuvant chemotherapy; pancreatic cancer; pancreaticoduodenectomy.
© 2021 Wiley Periodicals LLC.
Figures
Comment in
-
Prognostic factors in patients with pancreatic ductal adenocarcinoma with neoadjuvant treatment and pancreatectomy.J Surg Oncol. 2022 May;125(6):1071. doi: 10.1002/jso.26819. Epub 2022 Mar 10. J Surg Oncol. 2022. PMID: 35267194 No abstract available.
References
-
- Siegel RL, Miller KD, Jemal A.: Cancer statistics, 2018. CA Cancer J Clin. 2018;68:7–30. - PubMed
-
- Conroy T, Hammel P, Hebbar M, et al. : FOLFIRINOX or gemcitabine as adjuvant therapy for pancreatic cancer. N Engl J Med 2018;379:2395–2406. - PubMed
-
- Merkow RP, Bilimoria KY, Tomlinson JS, et al. : Postoperative complications reduce adjuvant chemotherapy use in resectable pancreatic cancer. Ann Surg 2014;260:372–377. - PubMed
-
- Neoptolemos JP, Palmer DH, Ghaneh P, et al. : Comparison of adjuvant gemcitabine and capecitabine with gemcitabine monotherapy in patients with resected pancreatic cancer (ESPAC-4): A multicentre, open-label, randomised, phase 3 trial. Lancet 2017;389:1011–1024. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
