

Distinct cytokine profiles associated with COVID-19 severity and mortality
- PMID: 33894209
- PMCID: PMC8061091
- DOI: 10.1016/j.jaci.2021.03.047
Distinct cytokine profiles associated with COVID-19 severity and mortality
Abstract
Background: Markedly elevated levels of proinflammatory cytokines and defective type-I interferon responses were reported in patients with coronavirus disease 2019 (COVID-19).
Objective: We sought to determine whether particular cytokine profiles are associated with COVID-19 severity and mortality.
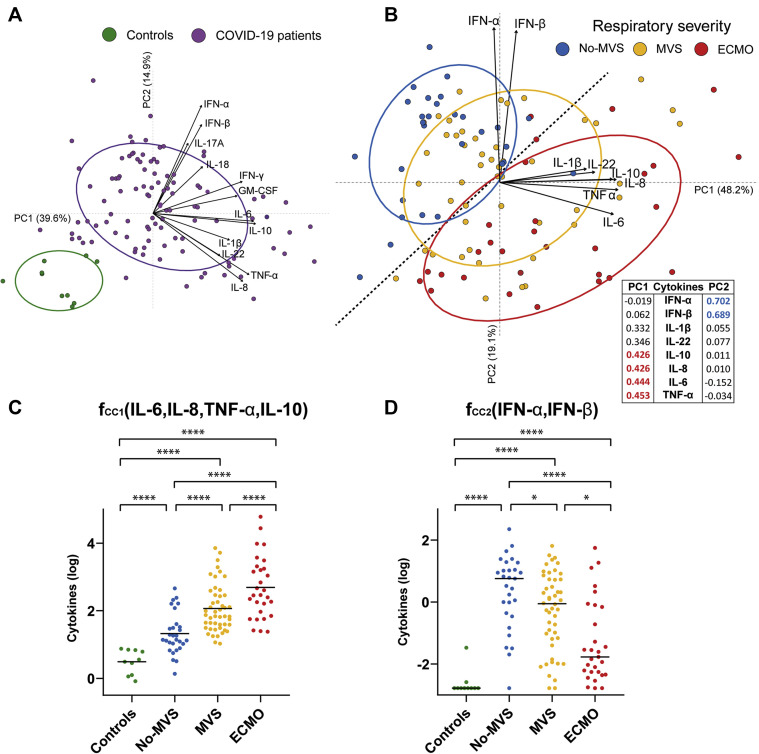
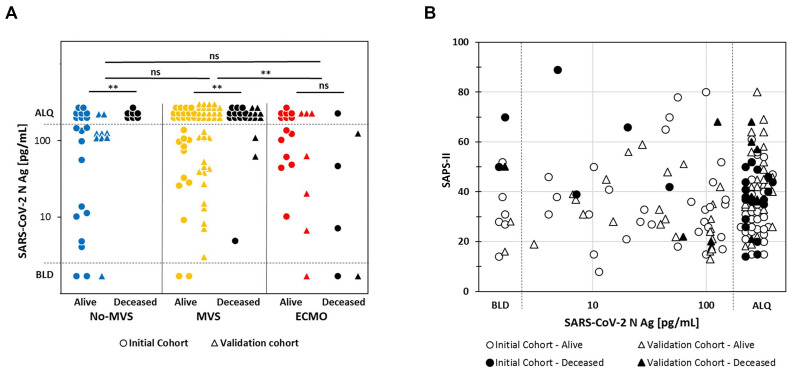
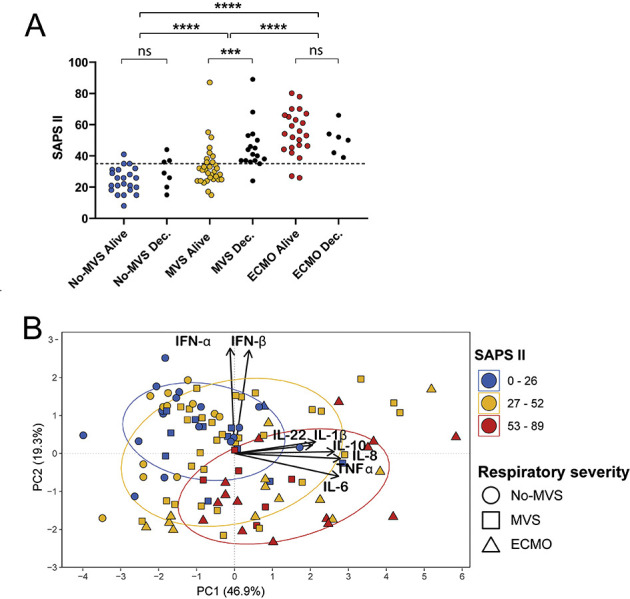
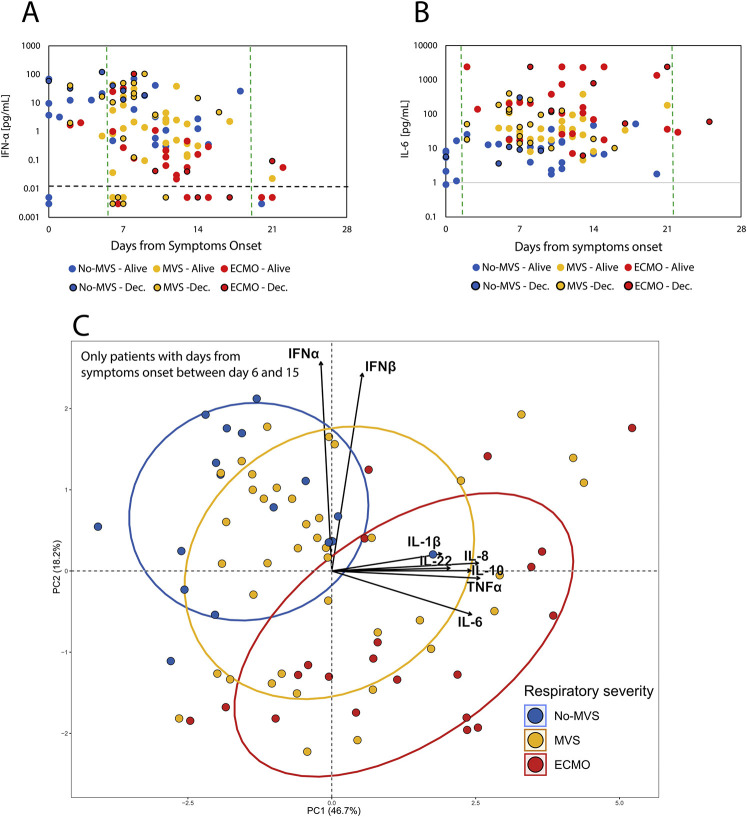
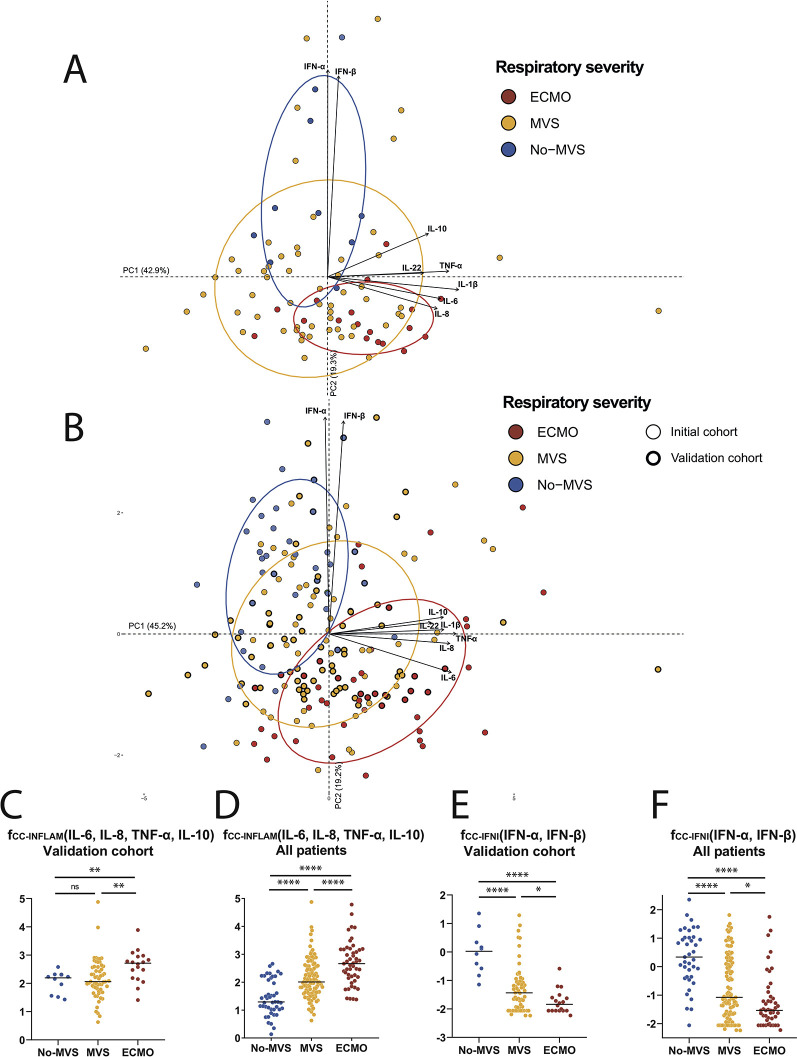
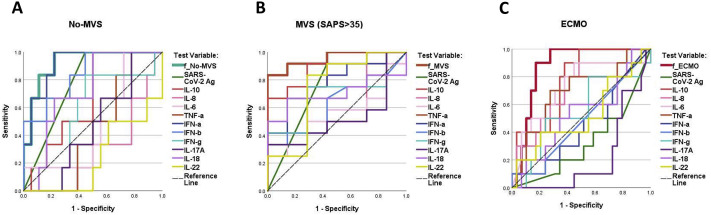
Methods: Cytokine concentrations and severe acute respiratory syndrome coronavirus 2 antigen were measured at hospital admission in serum of symptomatic patients with COVID-19 (N = 115), classified at hospitalization into 3 respiratory severity groups: no need for mechanical ventilatory support (No-MVS), intermediate severity requiring mechanical ventilatory support (MVS), and critical severity requiring extracorporeal membrane oxygenation (ECMO). Principal-component analysis was used to characterize cytokine profiles associated with severity and mortality. The results were thereafter confirmed in an independent validation cohort (N = 86).
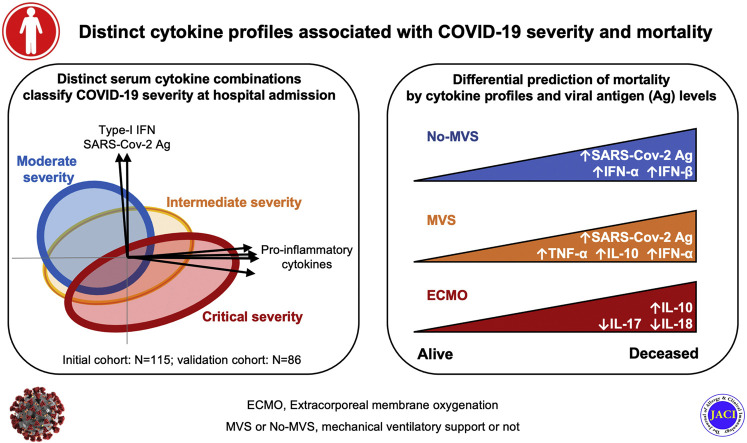
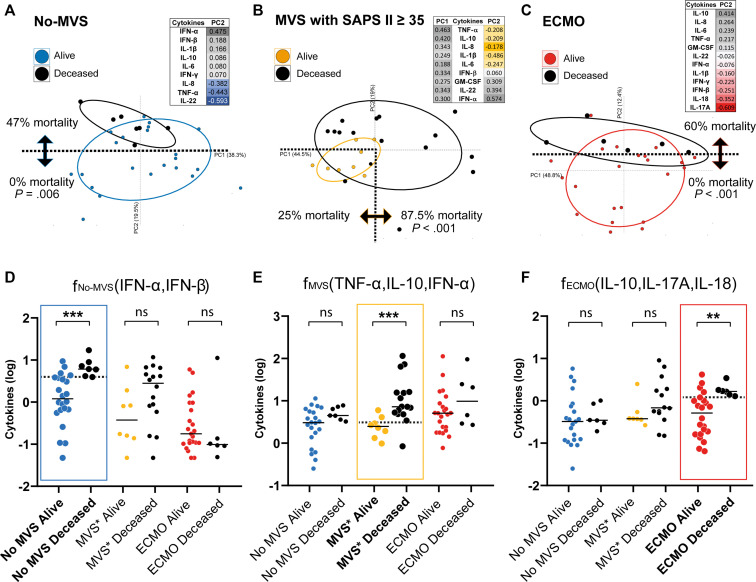
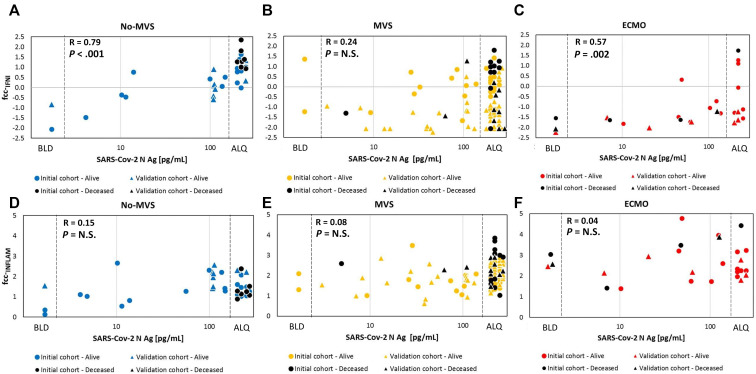
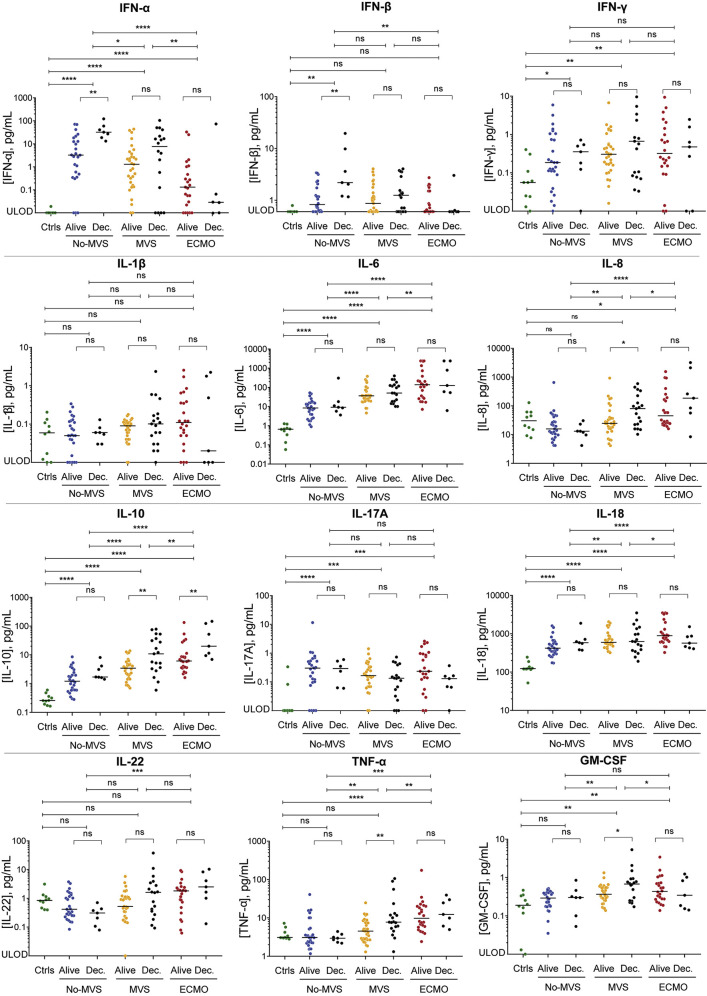
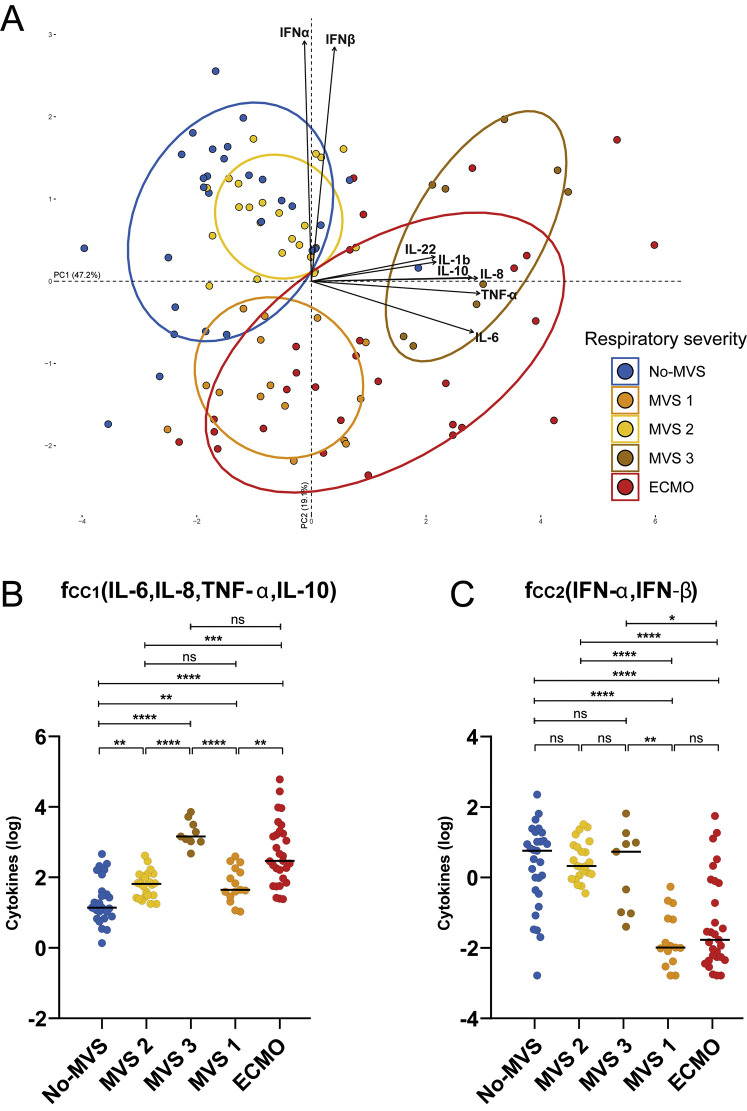
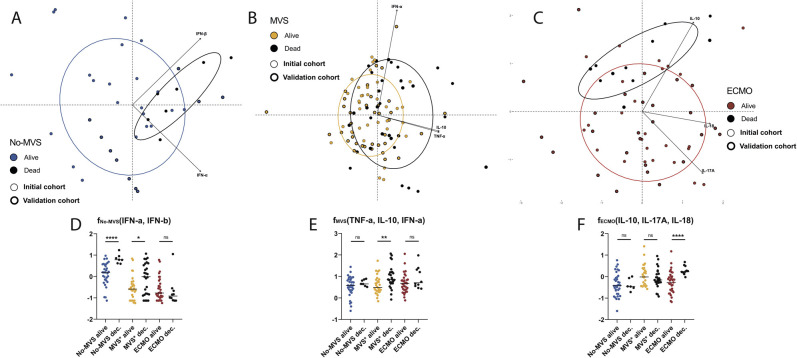
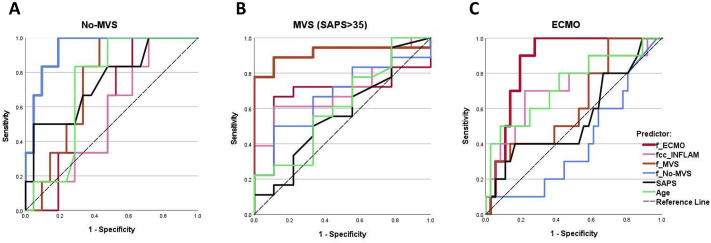
Results: At time of hospitalization, ECMO patients presented a dominant proinflammatory response with elevated levels of TNF-α, IL-6, IL-8, and IL-10. In contrast, an elevated type-I interferon response involving IFN-α and IFN-β was characteristic of No-MVS patients, whereas MVS patients exhibited both profiles. Mortality at 1 month was associated with higher levels of proinflammatory cytokines in ECMO patients, higher levels of type-I interferons in No-MVS patients, and their combination in MVS patients, resulting in a combined mortality prediction accuracy of 88.5% (risk ratio, 24.3; P < .0001). Severe acute respiratory syndrome coronavirus 2 antigen levels correlated with type-I interferon levels and were associated with mortality, but not with proinflammatory response or severity.
Conclusions: Distinct cytokine profiles are observed in association with COVID-19 severity and are differentially predictive of mortality according to oxygen support modalities. These results warrant personalized treatment of COVID-19 patients based on cytokine profiling.
Keywords: COVID-19; mortality; principal-component analysis; respiratory severity; serum cytokines; type-I interferons.
Copyright © 2021 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
