

[Evaluation of treatment with intra-articular injections in osteoarticular pathology of the shoulder in primary care]
- PMID: 33895613
- PMCID: PMC8093412
- DOI: 10.1016/j.aprim.2021.102051
[Evaluation of treatment with intra-articular injections in osteoarticular pathology of the shoulder in primary care]
Abstract
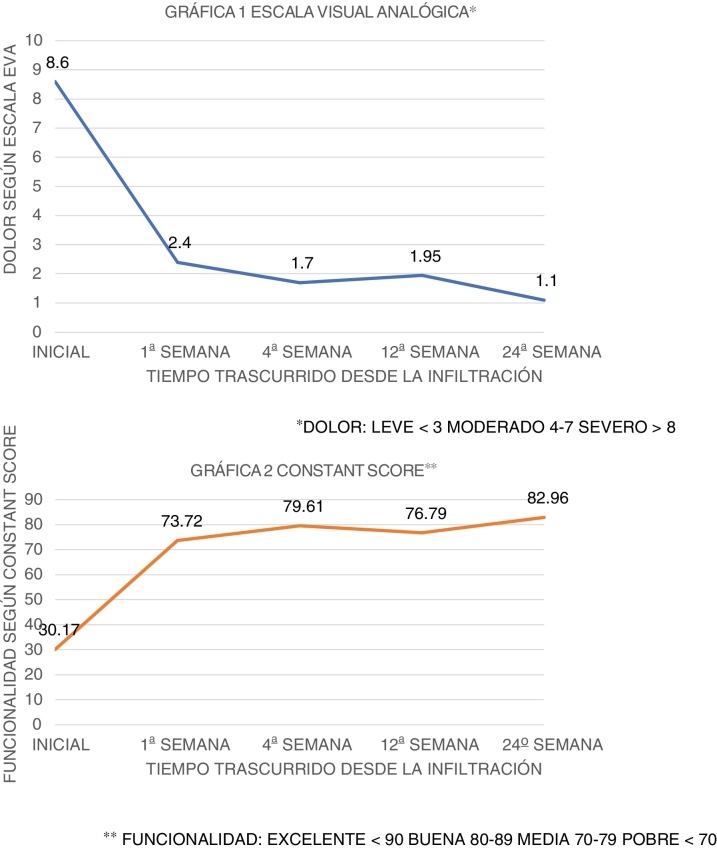
Main objective: To evaluate the clinical response at 24weeks after injection, measured as pain relief and functional recovery, in painful shoulder syndrome (PSS) in primary care (PC).
Design: Longitudinal case series with injection treatment in the scapulohumeral joint, describing functionality and pain evolution before and at 24weeks post injection.
Location: Non-urban primary care centres.
Participants: Patients with osteoarticular shoulder pathology susceptible to injection, failure of pharmacological treatment and rating on the visual analogue scale (VAS) ≥4 or constant score (CS) ≤70.
Interventions: Intra-articular injection of corticosteroid and local anaesthetic into the scapulohumeral joint, describing its evolution at 1, 4, 12 and 24weeks post injection.
Main measurements: Infiltration response according to EVA before and after, CS before and after, number of infiltrations, side effects, temporary inability to work (TIL).
Results: Sixty-six patients receiving injection, mean age 51.1years (SD 14.7), 57.6% were women and 63.3% were injection in the right shoulder. A 22.7% required TIL and were discharged with a median of 14days (range 7-56days). They required an injection (80.3%) and the most frequent injection pathology was rotator cuff tendinitis (90.9%). They suffered mild side effects (9.4%). We found a decrease in pain from severe to mild and a functional improvement from poor to good. The variables: being retired (OR: 37.82, P=.001) and having an EVA score prior to injection >8 (OR: 15.67, P=.055, almost significant) were associated with poor response.
Conclusions: Intra-articular administration of corticosteroids in PSS reduces pain and provides functional improvement after the first week after injection, and is maintained in the long term. This allows a quick recovery to work after an injection at two weeks reducing recovery time by 50%, with few side effects.
Objetivo principal: Evaluar la respuesta clínica a las 24 semanas de la infiltración, medida como alivio del dolor y recuperación funcional, en el síndrome de hombro doloroso (SHD) en atención primaria (AP).
Diseño: Serie de casos longitudinal con tratamiento de inyección en la articulación escapulohumeral; se describen la funcionalidad y la evolución del dolor previa y a las 24 semanas postinfiltración.
Emplazamiento: Atención Primaria. Centro de salud no urbano.
Participantes: Pacientes con patología osteoarticular de hombro susceptible de infiltración, fracaso de tratamiento farmacológico y calificación en la escala analógica visual (EVA) ≥ 4 o Constant Score (CS) ≤ 70.
Intervenciones: Inyección intraarticular corticosteroide y anestésico local en la articulación escapulohumeral, describiendo su evolución a 1, 4, 12 y 24 semanas postinfiltración.
Mediciones principales: Respuesta de la infiltración según EVA antes-después, CS antes-después, número de infiltraciones, efectos secundarios, incapacidad laboral transitoria (ILT).
Resultados: Se infiltraron 66 pacientes, edad media 51,1 años (DE: 14,7), 57,6% mujeres, 63,3% infiltración hombro derecho. El 22,7% precisaron ILT y cursaron alta con una mediana de 14 días (rango de 7-56 días). Precisaron una infiltración (80,3%) y la patología infiltrada más frecuente fue la tendinitis de los rotadores (90,9%). Sufrieron efectos secundarios leves un 9,4%. Encontramos disminución de dolor de severo a leve y una mejoría funcional de pobre a buena. Las variables: ser jubilado (OR: 37,82, p = 0,001) y tener un puntaje EVA previo a la infiltración > 8 (OR; 15,67, p = 0,055, cuasi significativo) se asociaron a mala respuesta.
Conclusiones: La administración intraarticular de corticosteroides en el SHD disminuye el dolor y aporta una mejoría funcional tras la primera semana postinfiltración, manteniéndose a largo plazo. Esto permite una rápida incorporación laboral con una infiltración a las 2 semanas, disminuyendo en un 50% el tiempo de recuperación, con escasos efectos secundarios.
Keywords: Atención primaria; Hombro doloroso; Intra-articular injections; Inyecciones intraarticulares; Primary care; Shoulder pain.
Copyright © 2021 The Authors. Publicado por Elsevier España, S.L.U. All rights reserved.
Figures
Similar articles
-
An Intra-articular Steroid Injection at 6 Weeks Postoperatively for Shoulder Stiffness After Arthroscopic Rotator Cuff Repair Does Not Affect Repair Integrity.Am J Sports Med. 2018 Jul;46(9):2192-2202. doi: 10.1177/0363546518777739. Epub 2018 Jun 20. Am J Sports Med. 2018. PMID: 29924633
-
Are intra-articular corticosteroid injections better than conventional TENS in treatment of rotator cuff tendinitis in the short run? A randomized study.Eur J Phys Rehabil Med. 2010 Sep;46(3):315-24. Epub 2010 Apr 13. Eur J Phys Rehabil Med. 2010. PMID: 20926997 Clinical Trial.
-
Intra-articular injection of steroids in the early postoperative period does not have an adverse effect on the clinical outcomes and the re-tear rate after arthroscopic rotator cuff repair.Knee Surg Sports Traumatol Arthrosc. 2019 Dec;27(12):3912-3919. doi: 10.1007/s00167-019-05486-3. Epub 2019 Apr 12. Knee Surg Sports Traumatol Arthrosc. 2019. PMID: 30980117
-
Systematic Review and Meta-Analysis of Nonoperative Platelet-Rich Plasma Shoulder Injections for Rotator Cuff Pathology.PM R. 2021 Oct;13(10):1157-1168. doi: 10.1002/pmrj.12516. Epub 2021 Jan 4. PM R. 2021. PMID: 33131197
-
A systematic review of randomized control trials looking at functional improvement of rotator cuff partial thickness tears following platelet-rich-plasma injection: a comparison of glenohumeral joint vs. subacromial bursa vs. intratendinous injection locations.JSES Int. 2024 Jan 24;8(3):464-471. doi: 10.1016/j.jseint.2024.01.003. eCollection 2024 May. JSES Int. 2024. PMID: 38707549 Free PMC article. Review.
Cited by
-
Joint Efforts: A Review of Large Joint and Bursa Steroid Injections and Aspirations by Primary Care Physicians.J Gen Intern Med. 2025 Apr 17. doi: 10.1007/s11606-025-09490-x. Online ahead of print. J Gen Intern Med. 2025. PMID: 40246753 Review.
-
The comparison of the efficacy of intramuscular tetracosactide and subacromial triamcinolone injection in rotator cuff tendinitis: a randomized trial.Rheumatol Adv Pract. 2024 Dec 20;9(1):rkae150. doi: 10.1093/rap/rkae150. eCollection 2025. Rheumatol Adv Pract. 2024. PMID: 39764362 Free PMC article.
-
[Short and long-term effectiveness of corticosterorid injections in osteoarticular pathology. Two-year Prospective Study].Aten Primaria. 2025 Mar 12;57(9):103250. doi: 10.1016/j.aprim.2025.103250. Online ahead of print. Aten Primaria. 2025. PMID: 40081315 Free PMC article. Spanish.
-
Effectiveness of Dry Needling and Ischemic Trigger Point Compression in the Gluteus Medius in Patients with Non-Specific Low Back Pain: A Randomized Short-Term Clinical Trial.Int J Environ Res Public Health. 2022 Sep 30;19(19):12468. doi: 10.3390/ijerph191912468. Int J Environ Res Public Health. 2022. PMID: 36231767 Free PMC article. Clinical Trial.
References
-
- Rodríguez-Martín S., Melogno-Klinkas M. El dolor crónico de hombro en las actividades instrumentales de la vida diaria. Rehabilitación. 2018;52:38–44.
-
- Green S., Buchbinder R., Hetrick S. Intervenciones fisioterapéuticas para el dolor del hombro. The Cochrane Library. 2008;1:65–75.
-
- Sanfélix J., Giner V., Fluixá C., Millán J., Fuertes A. Manual de infiltraciones en atención primaria. Generalitat. Conselleria de Sanitat. 2007 Disponible en: http://publicaciones.san.gva.es/publicaciones/documentos/V.5192-2007.pdf.
-
- Pfenninger J.L. Inyections of joints and soft tissue. Part I. General guidelines. Am Fam Physician. 1991;44:1196–1202. - PubMed
-
- Arteaga Domínguez A., García González C. Dolor de hombro: diferentes desórdenes y distintos tratamientos. Med Integr. 1999;34:393–402.
