

Impact and cost-effectiveness of potential interventions against infant respiratory syncytial virus (RSV) in 131 low-income and middle-income countries using a static cohort model
- PMID: 33895717
- PMCID: PMC8074564
- DOI: 10.1136/bmjopen-2020-046563
Impact and cost-effectiveness of potential interventions against infant respiratory syncytial virus (RSV) in 131 low-income and middle-income countries using a static cohort model
Abstract
Objectives: Interventions to prevent childhood respiratory syncytial virus (RSV) disease are limited and costly. New interventions are in advanced stages of development and could be available soon. This study aims to evaluate the potential impact and cost-effectiveness of two interventions to prevent childhood RSV-a maternal vaccine and a monoclonal antibody (mAb).
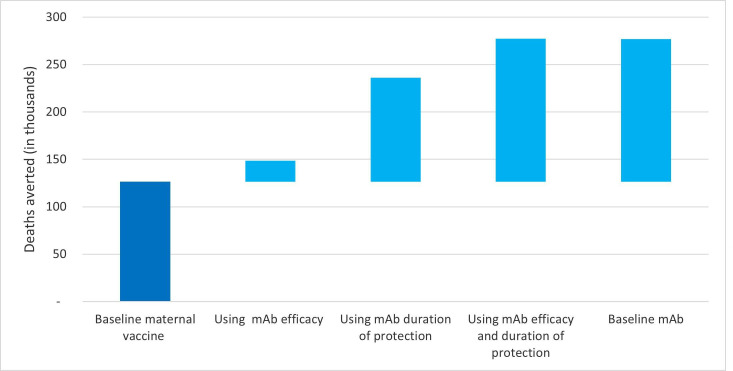
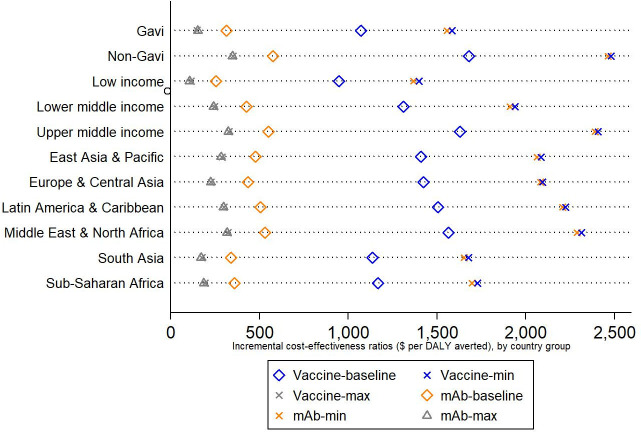
Design: Using a static population-based cohort model, we evaluate impact and cost-effectiveness of RSV interventions, from a health systems perspective. The assumed baseline efficacy and duration of protection were higher for the mAb (60%-70% efficacy, protection 6 months) compared with the maternal vaccine (40%-60% efficacy, protection 3 months). Both interventions were evaluated at US$3 and US$5 per dose for Gavi and non-Gavi countries, respectively. A range of input values were considered to explore uncertainty.
Settings: 131 low-income and middle-income countries.
Participants: Pregnant women and live birth cohorts.
Interventions: Maternal vaccine given to pregnant women and mAb given to young infants.
Primary and secondary outcome measures: Disability-adjusted life years averted, severe case averted, deaths averted, incremental cost effectiveness ratios.
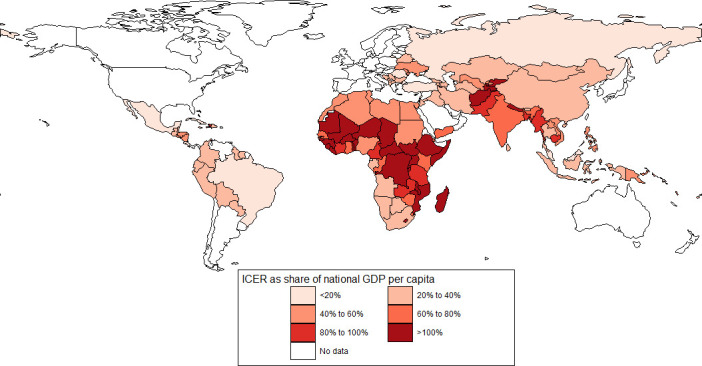
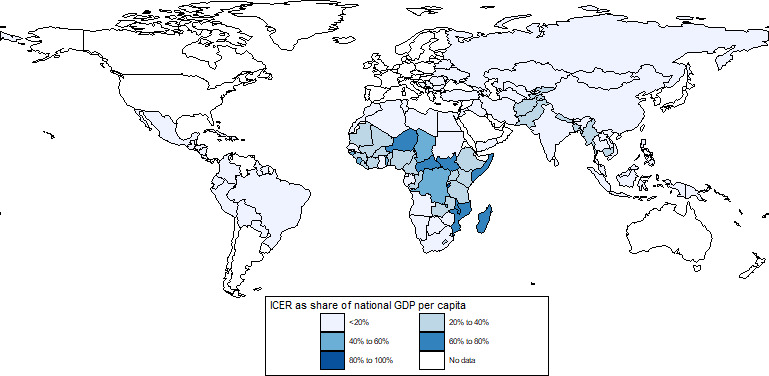
Results: Under baseline assumptions, maternal vaccine and mAbs were projected to avert 25% and 55% of RSV-related deaths among infants younger than 6 months of age, respectively. The average incremental cost-effectiveness ratio per disability-adjusted life year averted was US$1342 (range US$800-US$1866) for maternal RSV vaccine and US$431 (range US$167-US$692) for mAbs. At a 50% gross domestic product per capita threshold, maternal vaccine and mAbs were cost-effective in 60 and 118 countries, respectively.
Conclusions: Both interventions are projected to be impactful and cost-effective in many countries, a finding that would be enhanced if country-specific Gavi cofinancing to eligible countries were included. mAbs, with assumed higher efficacy and duration of protection, are expected to be more cost-effective than RSV maternal vaccines at similar prices. Final product characteristics will influence this finding.
Keywords: health economics; paediatrics; respiratory infections.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- GBD 2015 LRI Collaborators . Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory tract infections in 195 countries: a systematic analysis for the global burden of disease study 2015. Lancet Infect Dis 2017;17:1133–61. 10.1016/S1473-3099(17)30396-1 - DOI - PMC - PubMed
-
- Shi T, McAllister DA, O'Brien KL, et al. . Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet 2017;390:946–58. 10.1016/S0140-6736(17)30938-8 - DOI - PMC - PubMed
-
- Child Health and Mortality Prevention Surveillance (CHAMPS) [Internet], 2020. Available: https://champshealth.org/
-
- Utrecht University . News [Internet]. First consortium of local manufacturers to make affordable biosimilars available for low income countries, 2016. Available: https://www.uu.nl/en/news/first-consortium-of-local-manufacturers-to-mak...
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources