

Impact of Advanced Practice Provider Integration into Multispecialty Group Practices on Outcomes Following Major Surgery
- PMID: 33896274
- PMCID: PMC8542060
- DOI: 10.1177/15533506211013150
Impact of Advanced Practice Provider Integration into Multispecialty Group Practices on Outcomes Following Major Surgery
Abstract
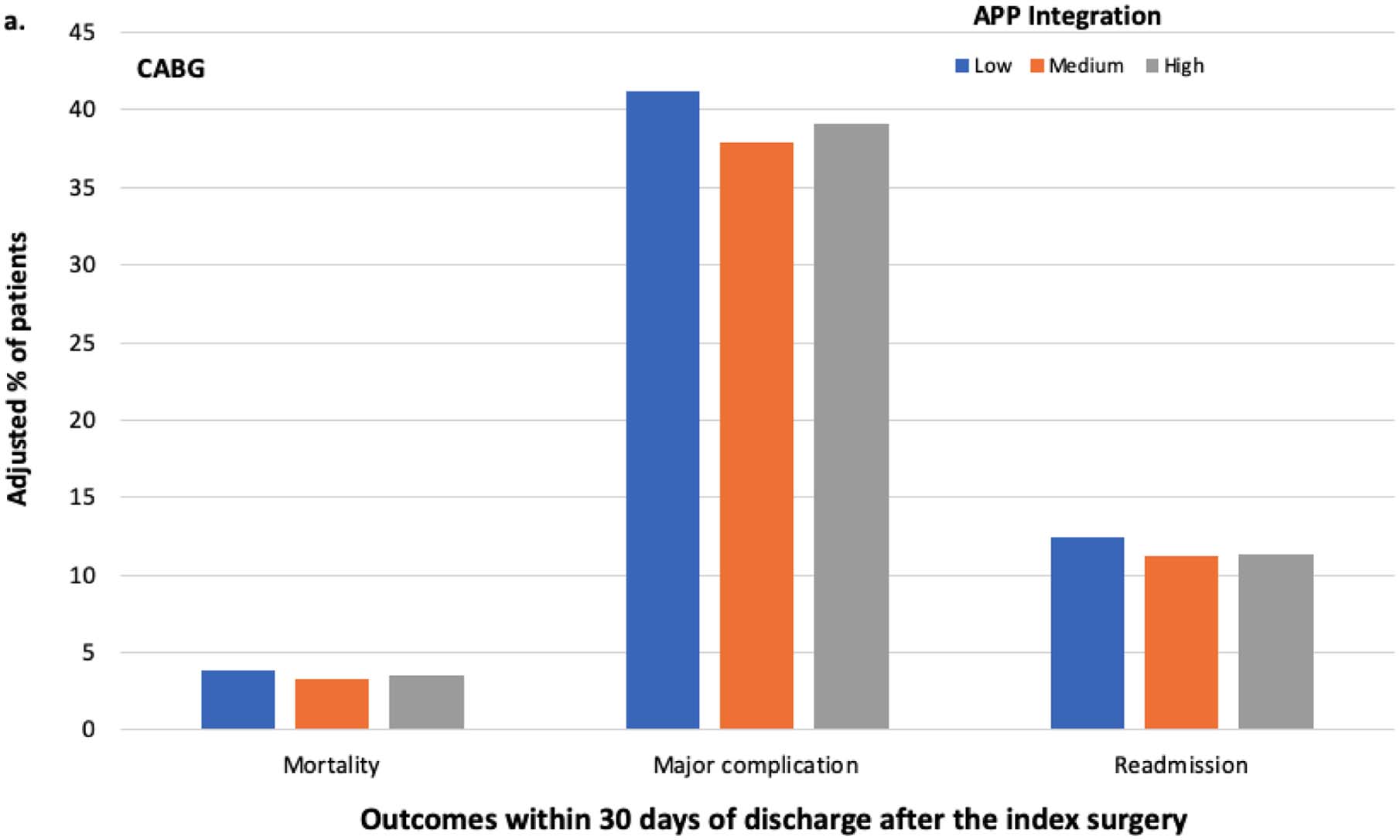
Background. While advanced practice providers (APPs) are increasingly integrated into care delivery models, little is known about their impact in surgical settings. Given that many patients undergo surgery in multispecialty group practice settings, we examined the impact of APP integration into such practices on outcomes after major surgery. Methods. We used a 20% sample of national Medicare claims to identify 190 101 patients who underwent 1 of 4 major surgeries (coronary artery bypass graft [CABG], colectomy, major joint replacement, and cystectomy) at multispecialty group practices from 2010 through 2016. The level of APP integration was measured as the ratio of APPs to physicians within each practice. Rates of mortality, major complications, and readmission within 30 days of discharge after the index surgery were compared between patients treated in practices with low, medium, and high levels of APP integration using multivariable regression analysis. Results. Relative to patients treated in practices with low APP integration, those treated in practices with medium or high APP integration had significantly lower rates of mortality (2.4% [low integration] vs 1.9% [medium integration] vs 2.0% [high integration]; P < .01), major complications (34.1% [low] vs 31.2% [medium] vs 30.2% [high]; P < .01), and readmission (11.7% [low] vs 10.6% [medium] vs 10.1% [high]; P < .01). This relationship was consistent for virtually all outcomes when considering each surgery type individually. Conclusions. Integration of APPs into multispecialty group practices was associated with improved postoperative outcomes after major surgery. Future research should identify the mechanisms by which APPs improve outcomes to inform optimal utilization.
Keywords: colorectal surgery; general surgery; surgical oncology; the business of surgery; urology.
Conflict of interest statement
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures




Similar articles
-
Effects of Advanced Practice Providers on Single-specialty Surgical Practice.Ann Surg. 2023 Jan 1;277(1):e40-e45. doi: 10.1097/SLA.0000000000004846. Epub 2021 Mar 3. Ann Surg. 2023. PMID: 33914476 Free PMC article.
-
Costs and Consequences of Early Hospital Discharge After Major Inpatient Surgery in Older Adults.JAMA Surg. 2017 May 17;152(5):e170123. doi: 10.1001/jamasurg.2017.0123. Epub 2017 May 17. JAMA Surg. 2017. PMID: 28329352 Free PMC article.
-
Impact of early discharge after coronary artery bypass graft surgery on rates of hospital readmission and death. The Ischemic Heart Disease (IHD) Patient Outcomes Research Team (PORT) Investigators.J Am Coll Cardiol. 1997 Oct;30(4):908-13. doi: 10.1016/s0735-1097(97)00243-x. J Am Coll Cardiol. 1997. PMID: 9316517
-
Stroke Rates Following Surgical Versus Percutaneous Coronary Revascularization.J Am Coll Cardiol. 2018 Jul 24;72(4):386-398. doi: 10.1016/j.jacc.2018.04.071. J Am Coll Cardiol. 2018. PMID: 30025574
-
Advancing the practice of trauma: utilizing advanced practice providers to improve patient outcomes through a collaborative team approach.Trauma Surg Acute Care Open. 2024 Aug 21;9(1):e001281. doi: 10.1136/tsaco-2023-001281. eCollection 2024. Trauma Surg Acute Care Open. 2024. PMID: 39175840 Free PMC article. Review.
Cited by
-
Integration of Advanced Practice Providers into Independent Surgical Groups.J Am Coll Surg. 2025 Aug 1:10.1097/XCS.0000000000001542. doi: 10.1097/XCS.0000000000001542. Online ahead of print. J Am Coll Surg. 2025. PMID: 40747891
-
Concurrent robotic colorectal surgical oncology training within a structured mentored international fellowship program.J Robot Surg. 2025 Mar 27;19(1):129. doi: 10.1007/s11701-025-02287-4. J Robot Surg. 2025. PMID: 40148715 Free PMC article.
References
-
- Bevis BLC, Berg-copas GM, Thomas W, et al. Outcomes of Tube Thoracostomies Performed by Advanced Practice Providers vs Trauma Surgeons. 2008;17(4):357–363. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
