

A deep learning pipeline for automatic analysis of multi-scan cardiovascular magnetic resonance
- PMID: 33896419
- PMCID: PMC8074440
- DOI: 10.1186/s12968-020-00695-z
A deep learning pipeline for automatic analysis of multi-scan cardiovascular magnetic resonance
Abstract
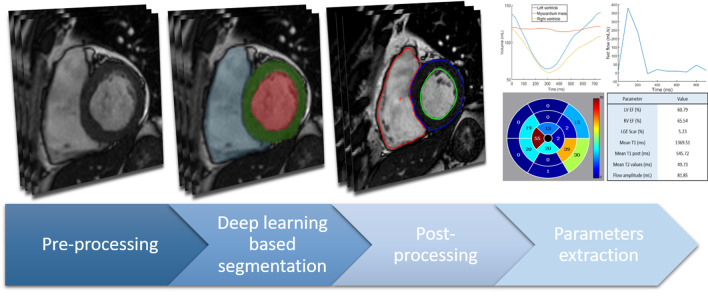
Background: Cardiovascular magnetic resonance (CMR) sequences are commonly used to obtain a complete description of the function and structure of the heart, provided that accurate measurements are extracted from images. New methods of extraction of information are being developed, among them, deep neural networks are powerful tools that showed the ability to perform fast and accurate segmentation. Iq1n order to reduce the time spent by reading physicians to process data and minimize intra- and inter-observer variability, we propose a fully automatic multi-scan CMR image analysis pipeline.
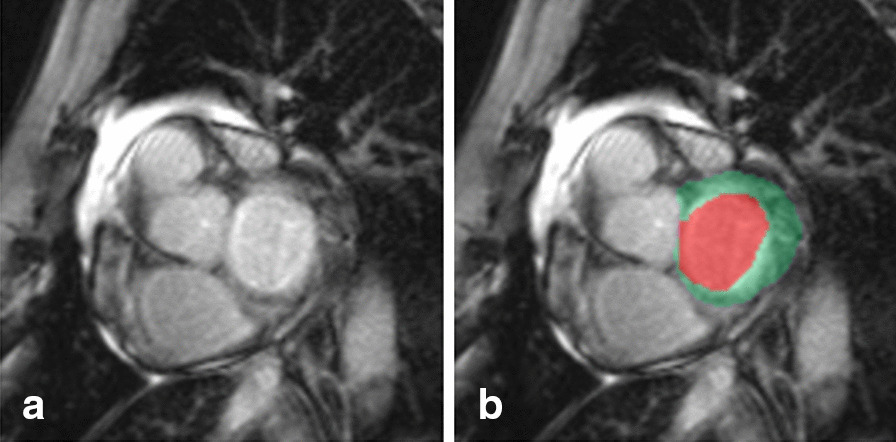
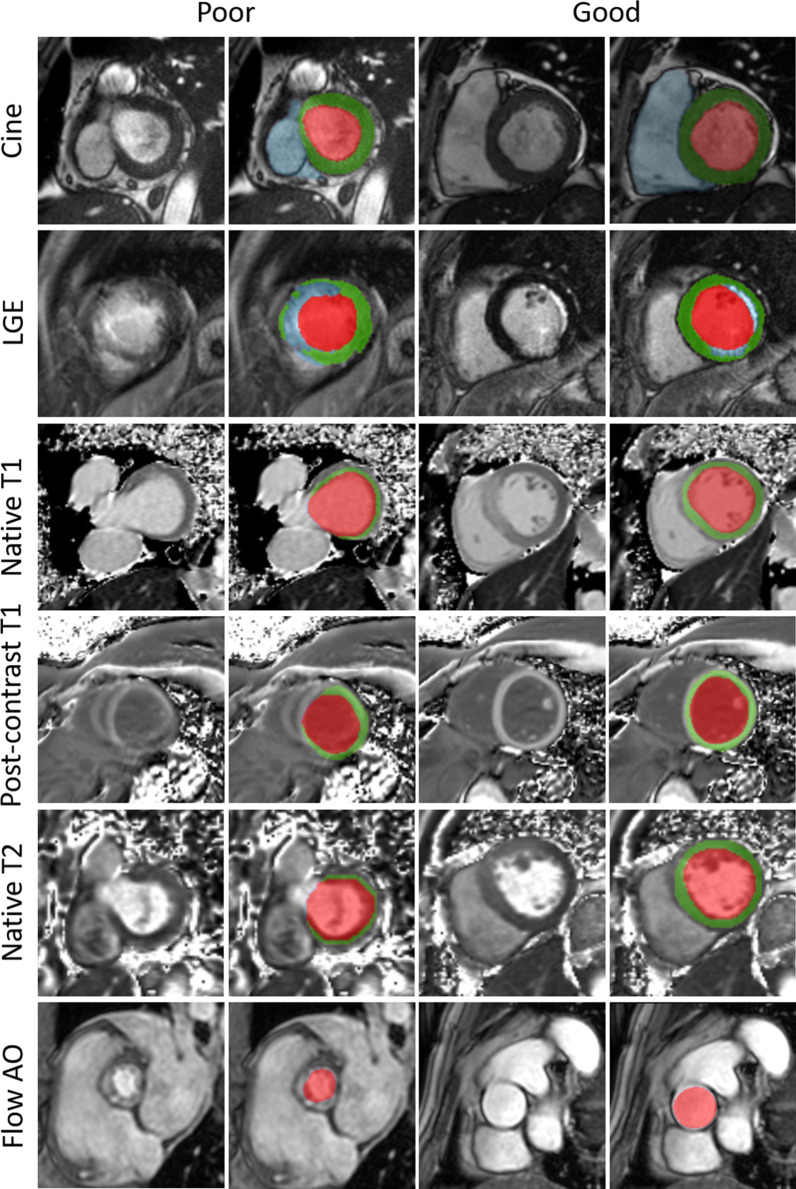
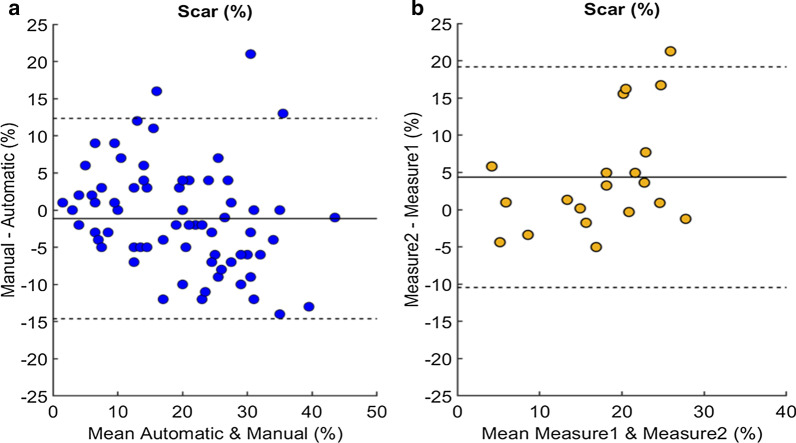
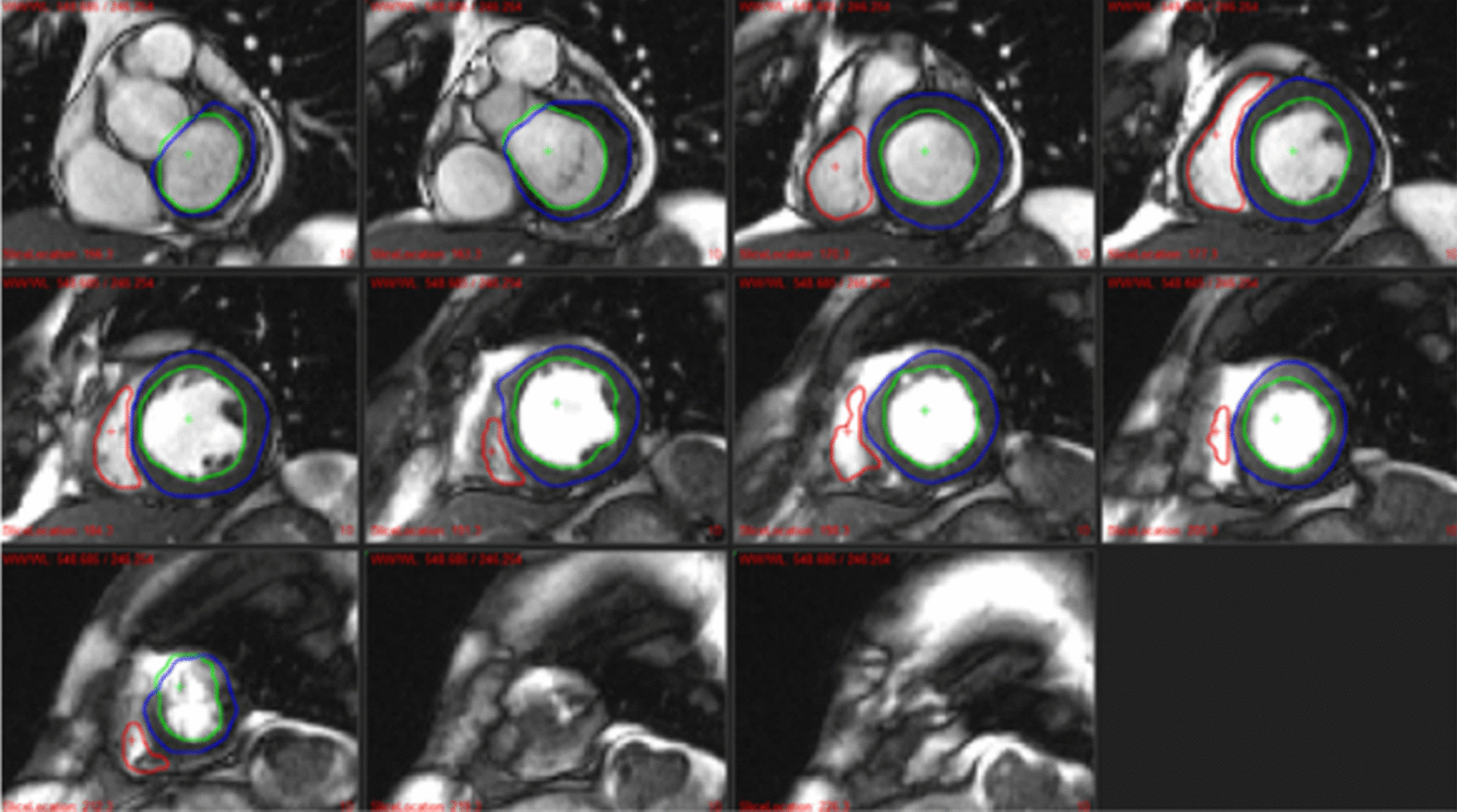
Methods: Sequence specific U-Net 2D models were trained to perform the segmentation of the left ventricle (LV), right ventricle (RV) and aorta in cine short-axis, late gadolinium enhancement (LGE), native T1 map, post-contrast T1, native T2 map and aortic flow sequences depending on the need. The models were trained and tested on a set of data manually segmented by experts using semi-automatic and manual tools. A set of parameters were computed from the resulting segmentations such as the left ventricular and right ventricular ejection fraction (EF), LGE scar percentage, the mean T1, T1 post, T2 values within the myocardium, and aortic flow. The Dice similarity coefficient, Hausdorff distance, mean surface distance, and Pearson correlation coefficient R were used to assess and compare the results of the U-Net based pipeline with intra-observer variability. Additionally, the pipeline was validated on two clinical studies.
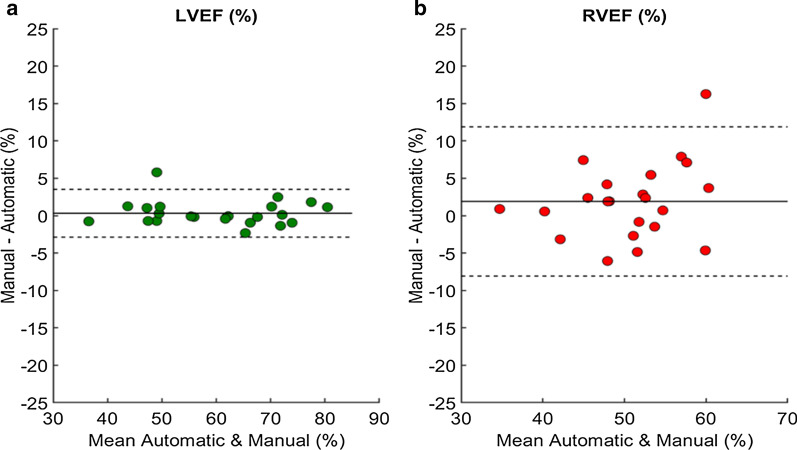
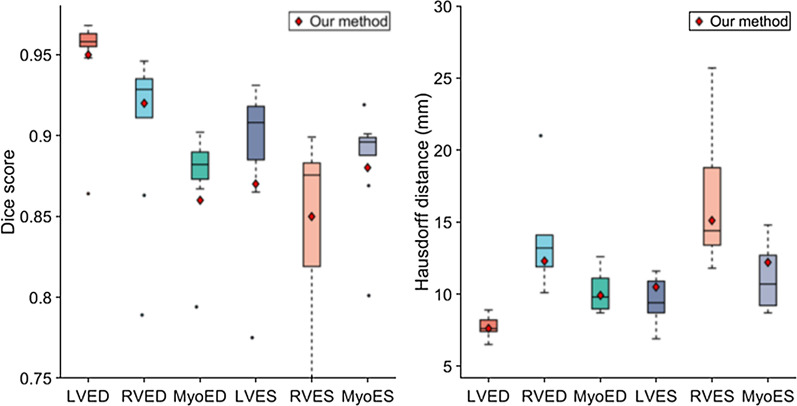
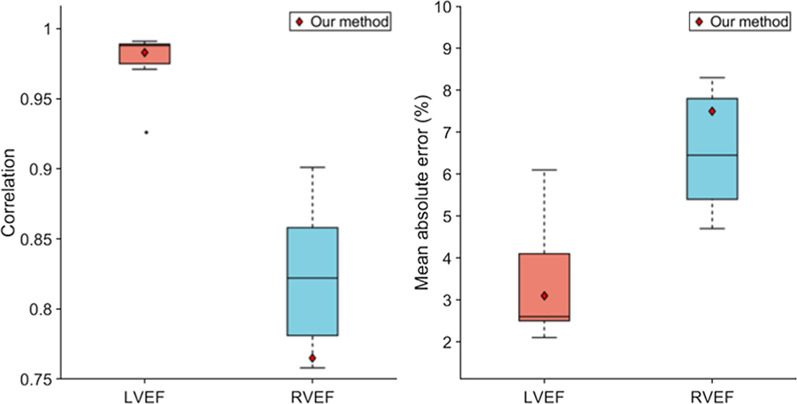
Results: The sequence specific U-Net 2D models trained achieved fast (≤ 0.2 s/image on GPU) and precise segmentation over all the targeted region of interest with high Dice scores (= 0.91 for LV, = 0.92 for RV, = 0.93 for Aorta in average) comparable to intra-observer Dice scores (= 0.86 for LV, = 0.87 for RV, = 0.95 for aorta flow in average). The automatically and manually computed parameters were highly correlated (R = 0.91 in average) showing results superior to the intra-observer variability (R = 0.85 in average) for every sequence presented here.
Conclusion: The proposed pipeline allows for fast and robust analysis of large CMR studies while guaranteeing reproducibility, hence potentially improving patient's diagnosis as well as clinical studies outcome.
Keywords: Aortic flow; Automatic analysis; Cine short-axis; Deep learning; Segmentation; T1 mapping; T2 mapping.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Bernard O, Lalande A, Zotti C, Cervenansky F, Yang X, Heng P-A, Cetin I, Lekadir K, Camara O, Ballester MAG, et al. Deep learning techniques for automatic mri cardiac multi-structures segmentation and diagnosis: Is the problem solved? IEEE Trans Med Imaging. 2018;99:1. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
