

Risk factors of non-union in Anderson-D'Alonzo type III odontoid fractures with conservative treatment
- PMID: 33897130
- PMCID: PMC8049875
- DOI: 10.1016/j.jor.2021.03.012
Risk factors of non-union in Anderson-D'Alonzo type III odontoid fractures with conservative treatment
Abstract
Objective: The purpose of this study was retrospectively to analyze the risk factors for non-union in Anderson-D'Alonzo type III odontoid fractures with conservative treatment.
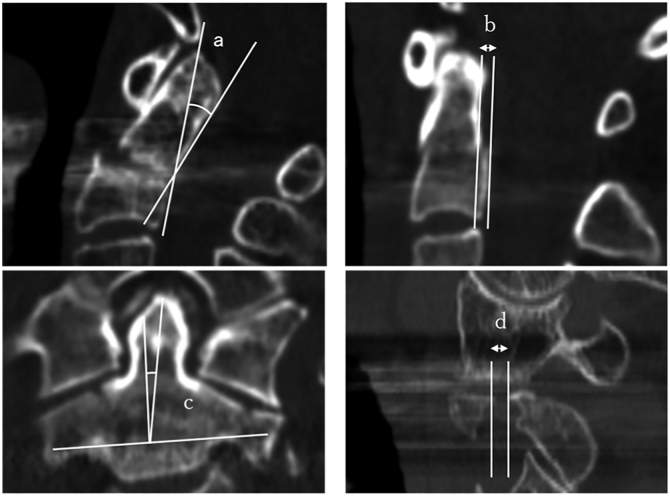
Methods: 25 patients with type III fractures were analyzed. Coronal and sagittal tilt as well as sagittal and lateral mass gaps were measured by using computed tomography.
Results: The non-union group had significantly higher age, greater coronal tilt and lateral mass gap. Especially, the lateral mass gap was >2 mm in all cases with non-union.
Conclusions: Higher age, coronal tilt, and lateral mass gap were significant risk factors for non-union.
Keywords: Anderson–D’Alonzo type III odontoid Fractures; Conservative treatment; Non-union; Risk factors.
© 2021 Professor P K Surendran Memorial Education Foundation. Published by Elsevier B.V. All rights reserved.
Figures

Similar articles
-
Comparison of Atlantoaxial Rotation and Functional Outcomes of Two Nonfusion Techniques in the Treatment of Anderson-D'Alonzo Type II Odontoid Fractures.Spine (Phila Pa 1976). 2016 Jun;41(12):E751-E758. doi: 10.1097/BRS.0000000000001370. Spine (Phila Pa 1976). 2016. PMID: 26656043
-
[Anterior osteosynthesis of odontoid fractures].Acta Chir Orthop Traumatol Cech. 2008 Oct;75(5):332-8. Acta Chir Orthop Traumatol Cech. 2008. PMID: 19026186 Czech.
-
[Cement-augmented anterior odontoid screw fixation of a Anderson-D'Alonzo type II fracture with massive osteoporosis. Case report].Z Orthop Unfall. 2011 Jun;149(3):308-11. doi: 10.1055/s-0030-1250686. Epub 2011 Feb 8. Z Orthop Unfall. 2011. PMID: 21305453 German.
-
Odontoid Fractures: A Review of the Current State of the Art.J Clin Med. 2024 Oct 21;13(20):6270. doi: 10.3390/jcm13206270. J Clin Med. 2024. PMID: 39458221 Free PMC article. Review.
-
Surgical management of odontoid fractures.Injury. 2005 Jul;36 Suppl 2:B54-64. doi: 10.1016/j.injury.2005.06.015. Injury. 2005. PMID: 15993118 Review.
Cited by
-
Addressing the challenges of complex type III odontoid fractures: Clinical and radiological outcomes of various treatment modalities.J Orthop. 2024 Aug 18;60:10-18. doi: 10.1016/j.jor.2024.08.010. eCollection 2025 Feb. J Orthop. 2024. PMID: 39345681
-
Posterior wiring with sublaminar polyester bands, titanium-peek fixation system for C2 fracture management: a 4-patient case series with a maximum of 18 months' follow-up.J Spine Surg. 2023 Sep 22;9(3):306-313. doi: 10.21037/jss-22-77. Epub 2023 Aug 24. J Spine Surg. 2023. PMID: 37841786 Free PMC article.
-
Odontoid fractures in the pediatric population: a systematic review and management algorithm.J Child Orthop. 2024 Sep 19;18(5):486-494. doi: 10.1177/18632521241283232. eCollection 2024 Oct. J Child Orthop. 2024. PMID: 39391580 Free PMC article. Review.
References
-
- Ryan M.D., Henderson J.J. The epidemiology of fractures and fracture-dislocations of the cervical spine. Injury. 1992;23:38–40. - PubMed
-
- Anderson L.D., D'Alonzo R.T. Fractures of the odontoid process of the axis. J Bone Jt Surg Am Vol. 1974;56:1663–1674. - PubMed
-
- Grasso G., Leone L., Torregrossa F. Management of odontoid cervical fracture. World Neurosurg. 2019;123:246–247. - PubMed
-
- Iyer S., Hurlbert R.J., Albert T.J. Management of odontoid fractures in the elderly: a review of the literature and an evidence-based treatment algorithm. Neurosurgery. 2017;82:419–430. - PubMed
-
- Clark C.R., White A.A., 3rd Fractures of the dens. A multicenter study. J Bone Joint Surg Am. 1985;67:1340–1348. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
