

An Early Warning Tool for Predicting Mortality Risk of COVID-19 Patients Using Machine Learning
- PMID: 33897907
- PMCID: PMC8058759
- DOI: 10.1007/s12559-020-09812-7
An Early Warning Tool for Predicting Mortality Risk of COVID-19 Patients Using Machine Learning
Abstract
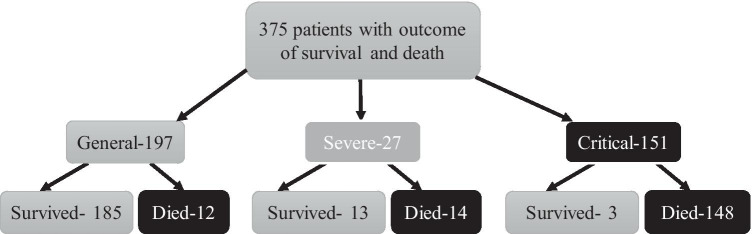
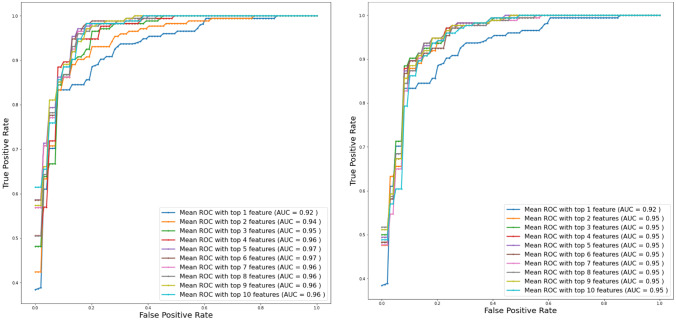
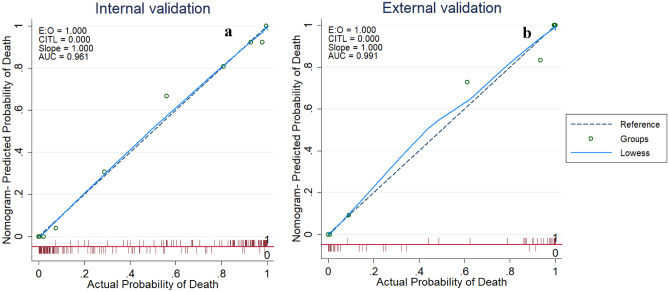
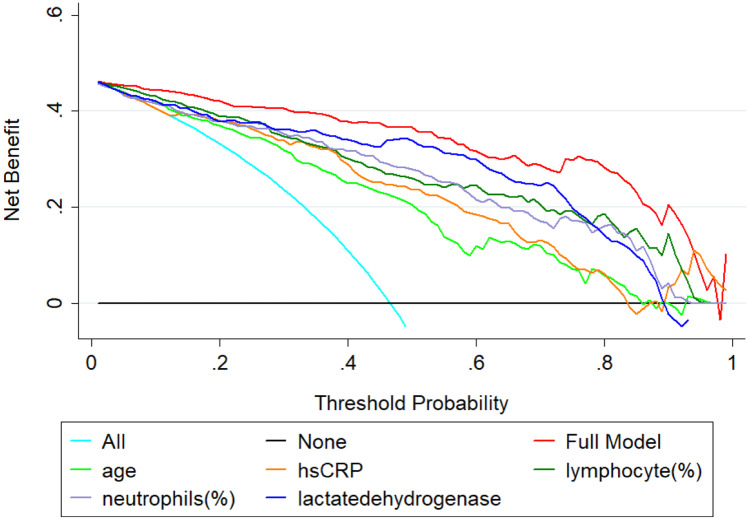
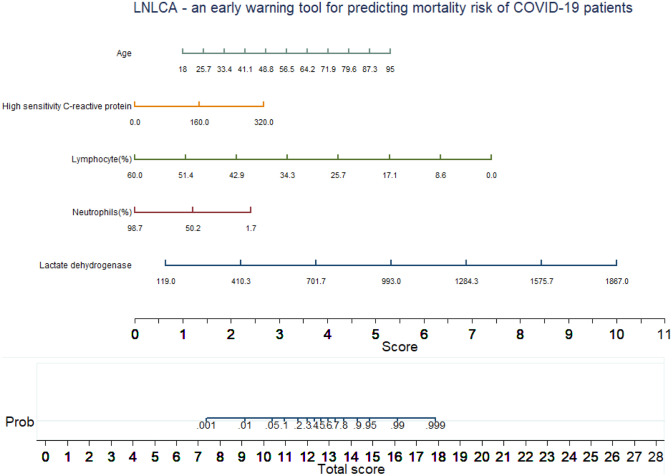
COVID-19 pandemic has created an extreme pressure on the global healthcare services. Fast, reliable, and early clinical assessment of the severity of the disease can help in allocating and prioritizing resources to reduce mortality. In order to study the important blood biomarkers for predicting disease mortality, a retrospective study was conducted on a dataset made public by Yan et al. in [1] of 375 COVID-19 positive patients admitted to Tongji Hospital (China) from January 10 to February 18, 2020. Demographic and clinical characteristics and patient outcomes were investigated using machine learning tools to identify key biomarkers to predict the mortality of individual patient. A nomogram was developed for predicting the mortality risk among COVID-19 patients. Lactate dehydrogenase, neutrophils (%), lymphocyte (%), high-sensitivity C-reactive protein, and age (LNLCA)-acquired at hospital admission-were identified as key predictors of death by multi-tree XGBoost model. The area under curve (AUC) of the nomogram for the derivation and validation cohort were 0.961 and 0.991, respectively. An integrated score (LNLCA) was calculated with the corresponding death probability. COVID-19 patients were divided into three subgroups: low-, moderate-, and high-risk groups using LNLCA cutoff values of 10.4 and 12.65 with the death probability less than 5%, 5-50%, and above 50%, respectively. The prognostic model, nomogram, and LNLCA score can help in early detection of high mortality risk of COVID-19 patients, which will help doctors to improve the management of patient stratification.
Keywords: COVID-19; Early warning tool; Machine learning; Predicting mortality risk; Prognostic model.
© The Author(s) 2021.
Conflict of interest statement
Conflict of InterestThe authors declare that they have no conflict of interest.
Figures


References
-
- Yan L, Zhang HT, Goncalves J, Xiao Y, Wang M, Guo Y, et al. "An interpretable mortality prediction model for COVID-19 patients. Nat Mach Intell. 2020: 1–6.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials