

Genome-Wide Association Study of Non-syndromic Orofacial Clefts in a Multiethnic Sample of Families and Controls Identifies Novel Regions
- PMID: 33898419
- PMCID: PMC8062975
- DOI: 10.3389/fcell.2021.621482
Genome-Wide Association Study of Non-syndromic Orofacial Clefts in a Multiethnic Sample of Families and Controls Identifies Novel Regions
Abstract
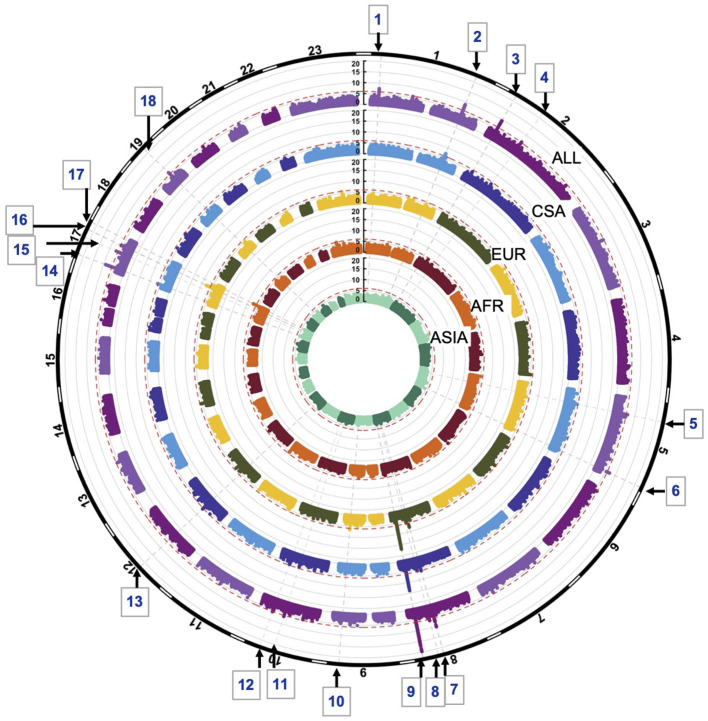
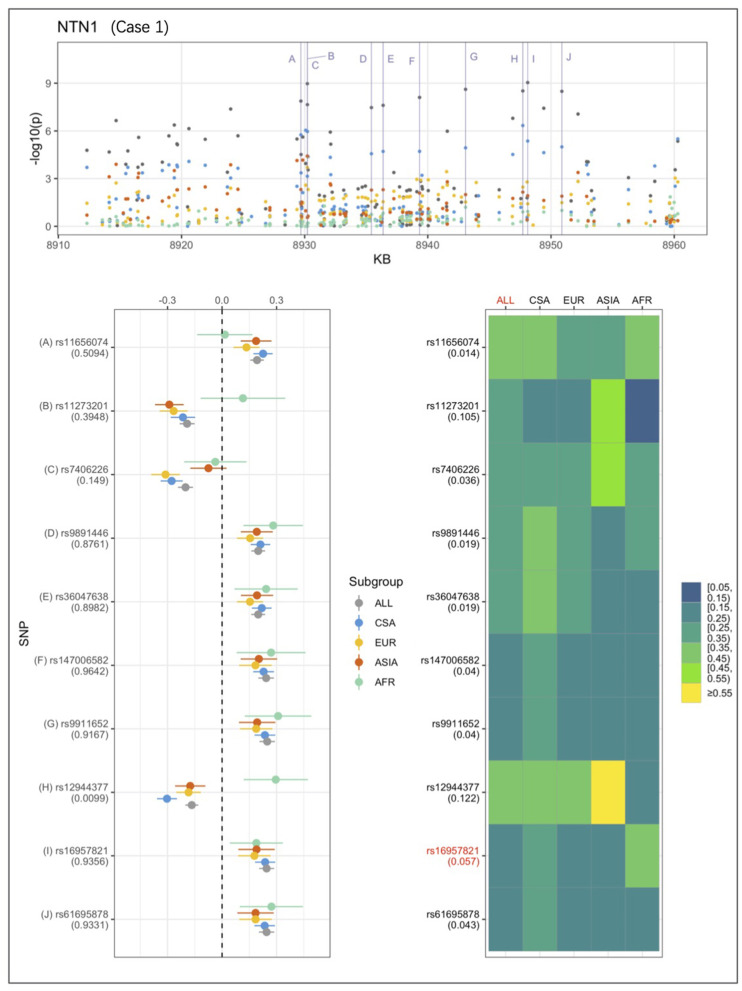
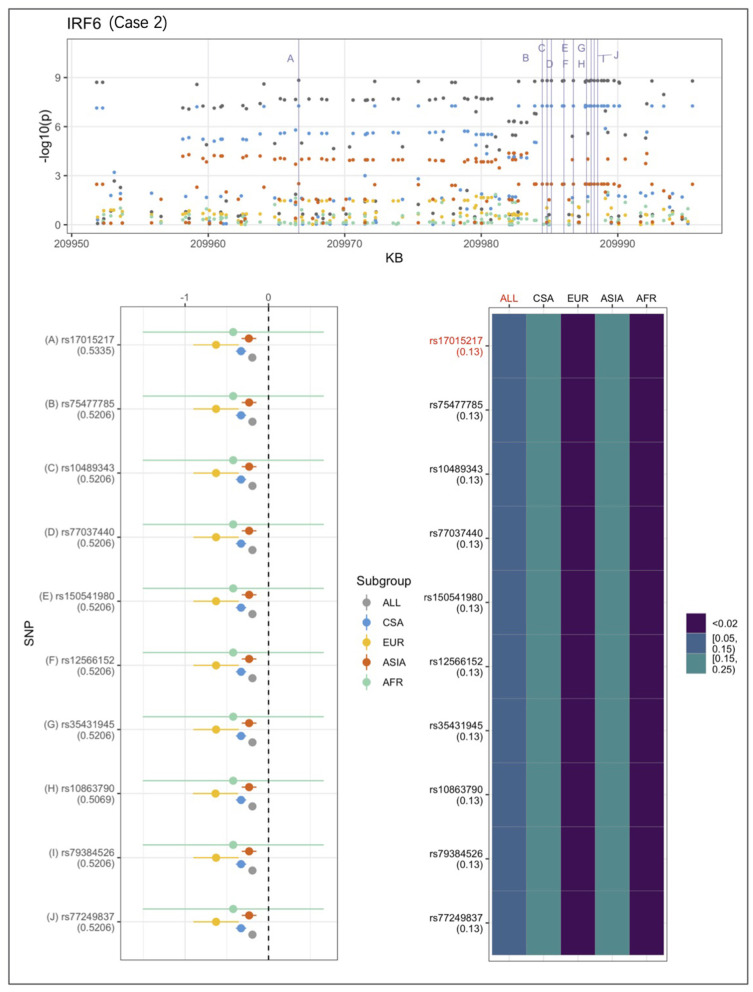
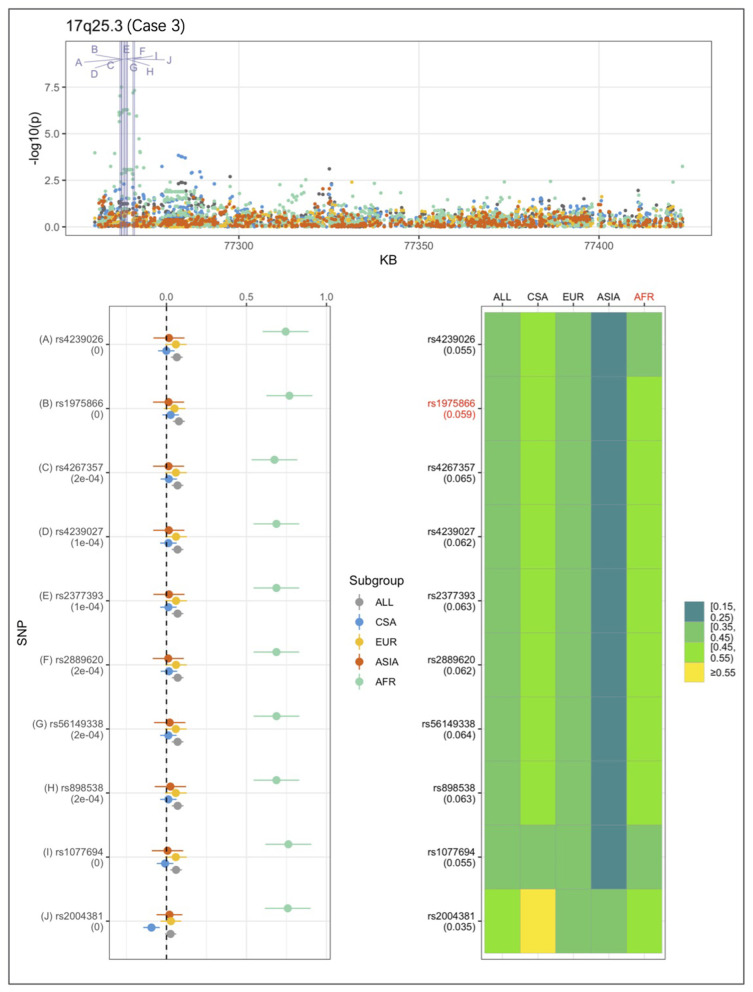
Orofacial clefts (OFCs) are among the most prevalent craniofacial birth defects worldwide and create a significant public health burden. The majority of OFCs are non-syndromic and vary in prevalence by ethnicity. Africans have the lowest prevalence of OFCs (~ 1/2,500), Asians have the highest prevalence (~1/500), Europeans and Latin Americans lie somewhere in the middle (~1/800 and 1/900, respectively). Thus, ethnicity appears to be a major determinant of the risk of developing OFC. The Pittsburgh Orofacial Clefts Multiethnic study was designed to explore this ethnic variance, comprising a large number of families and individuals (~12,000 individuals) from multiple populations worldwide: US and Europe, Asians, mixed Native American/Caucasians, and Africans. In this current study, we analyzed 2,915 OFC cases, 6,044 unaffected individuals related to the OFC cases, and 2,685 controls with no personal or family history of OFC. Participants were grouped by their ancestry into African, Asian, European, and Central and South American subsets, and genome-wide association run on the combined sample as well as the four ancestry-based groups. We observed 22 associations to cleft lip with or without cleft palate at 18 distinct loci with p-values < 1e-06, including 10 with genome-wide significance (<5e-08), in the combined sample and within ancestry groups. Three loci - 2p12 (rs62164740, p = 6.27e-07), 10q22.2 (rs150952246, p = 3.14e-07), and 10q24.32 (rs118107597, p = 8.21e-07) are novel. Nine were in or near known OFC loci - PAX7, IRF6, FAM49A, DCAF4L2, 8q24.21, NTN1, WNT3-WNT9B, TANC2, and RHPN2. The majority of the associations were observed only in the combined sample, European, and Central and South American groups. We investigated whether the observed differences in association strength were (a) purely due to sample sizes, (b) due to systematic allele frequency difference at the population level, or (c) due to the fact certain OFC-causing variants confer different amounts of risk depending on ancestral origin, by comparing effect sizes to observed allele frequencies of the effect allele in our ancestry-based groups. While some of the associations differ due to systematic differences in allele frequencies between groups, others show variation in effect size despite similar frequencies across ancestry groups.
Keywords: GWAS; family study; genetic factors in OFC; genetic heterogeneity; multiethnic.
Copyright © 2021 Mukhopadhyay, Feingold, Moreno-Uribe, Wehby, Valencia-Ramirez, Muñeton, Padilla, Deleyiannis, Christensen, Poletta, Orioli, Hecht, Buxó, Butali, Adeyemo, Vieira, Shaffer, Murray, Weinberg, Leslie and Marazita.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Grants and funding
- U54 GM133807/GM/NIGMS NIH HHS/United States
- R25 MD007607/MD/NIMHD NIH HHS/United States
- U54 MD007587/MD/NIMHD NIH HHS/United States
- S21 MD001830/MD/NIMHD NIH HHS/United States
- HHSN268201200008C/HL/NHLBI NIH HHS/United States
- U01 DE024425/DE/NIDCR NIH HHS/United States
- R21 DE016930/DE/NIDCR NIH HHS/United States
- R00 DE022378/DE/NIDCR NIH HHS/United States
- R01 DD000295/DD/NCBDD CDC HHS/United States
- R37 DE008559/DE/NIDCR NIH HHS/United States
- R01 DE011931/DE/NIDCR NIH HHS/United States
- R00 DE024571/DE/NIDCR NIH HHS/United States
- K99 DE022378/DE/NIDCR NIH HHS/United States
- R01 DE016148/DE/NIDCR NIH HHS/United States
- HHSN268201200008I/HL/NHLBI NIH HHS/United States
- R01 DE009886/DE/NIDCR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical