

Emerging strategies for treating metastasis
- PMID: 33899000
- PMCID: PMC8064405
- DOI: 10.1038/s43018-021-00181-0
Emerging strategies for treating metastasis
Abstract
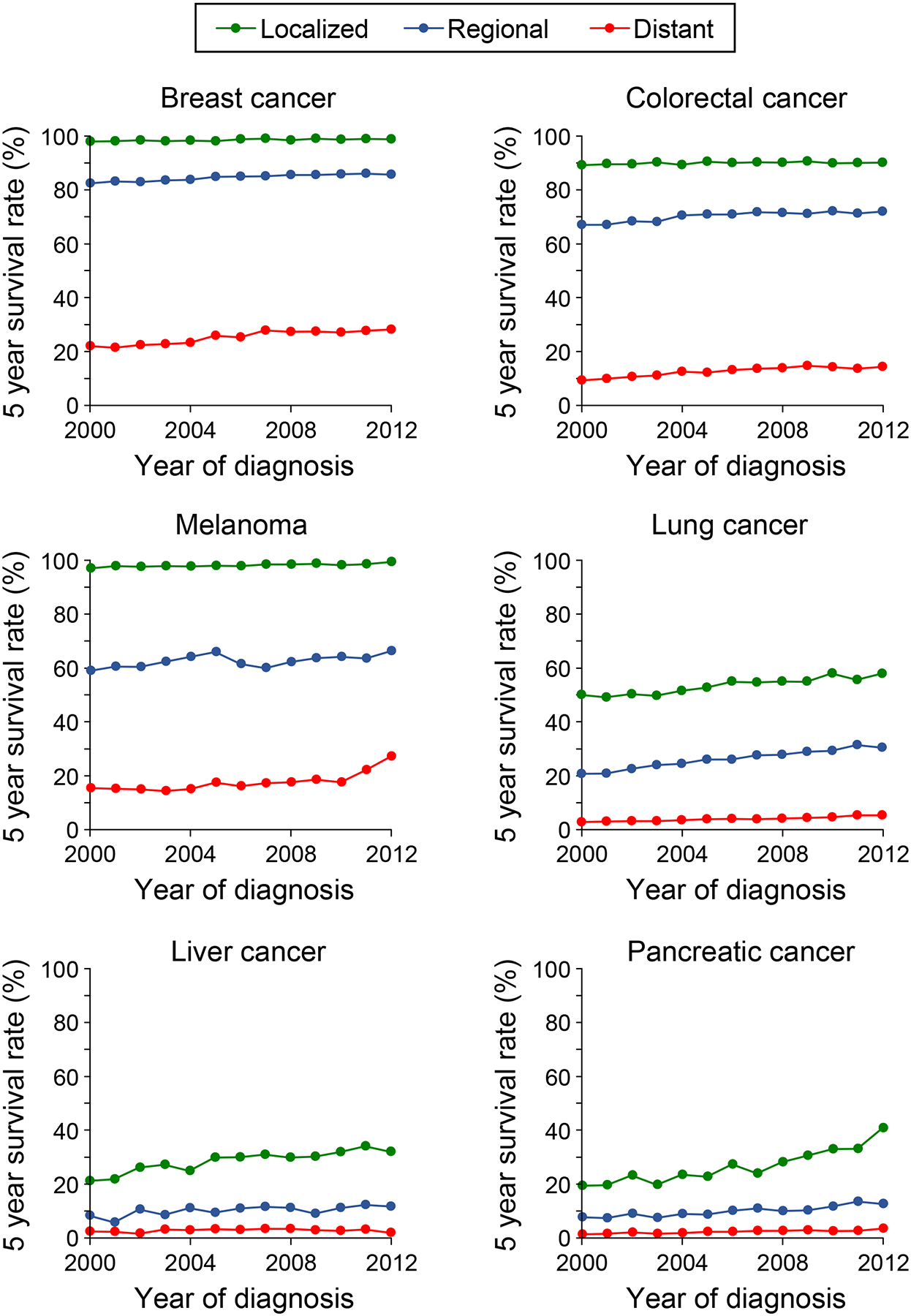
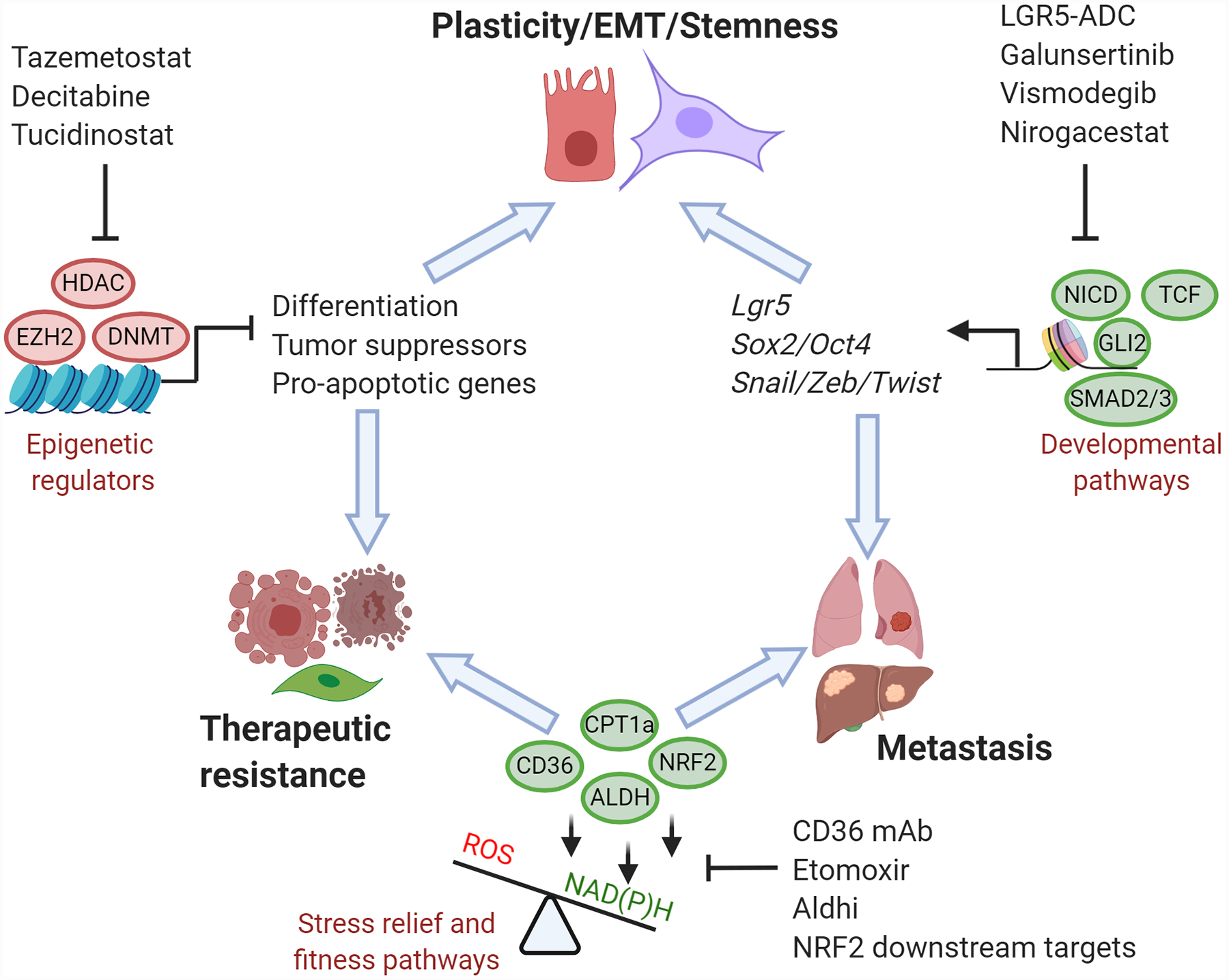
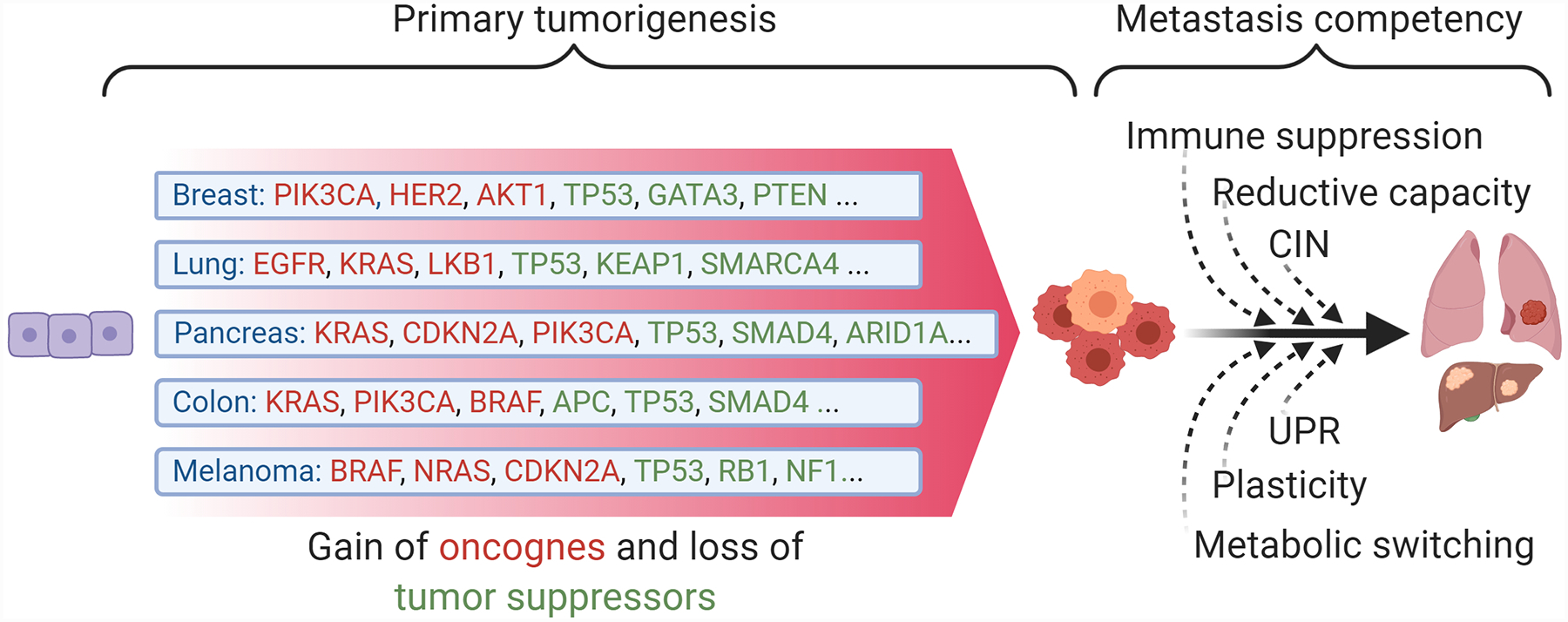
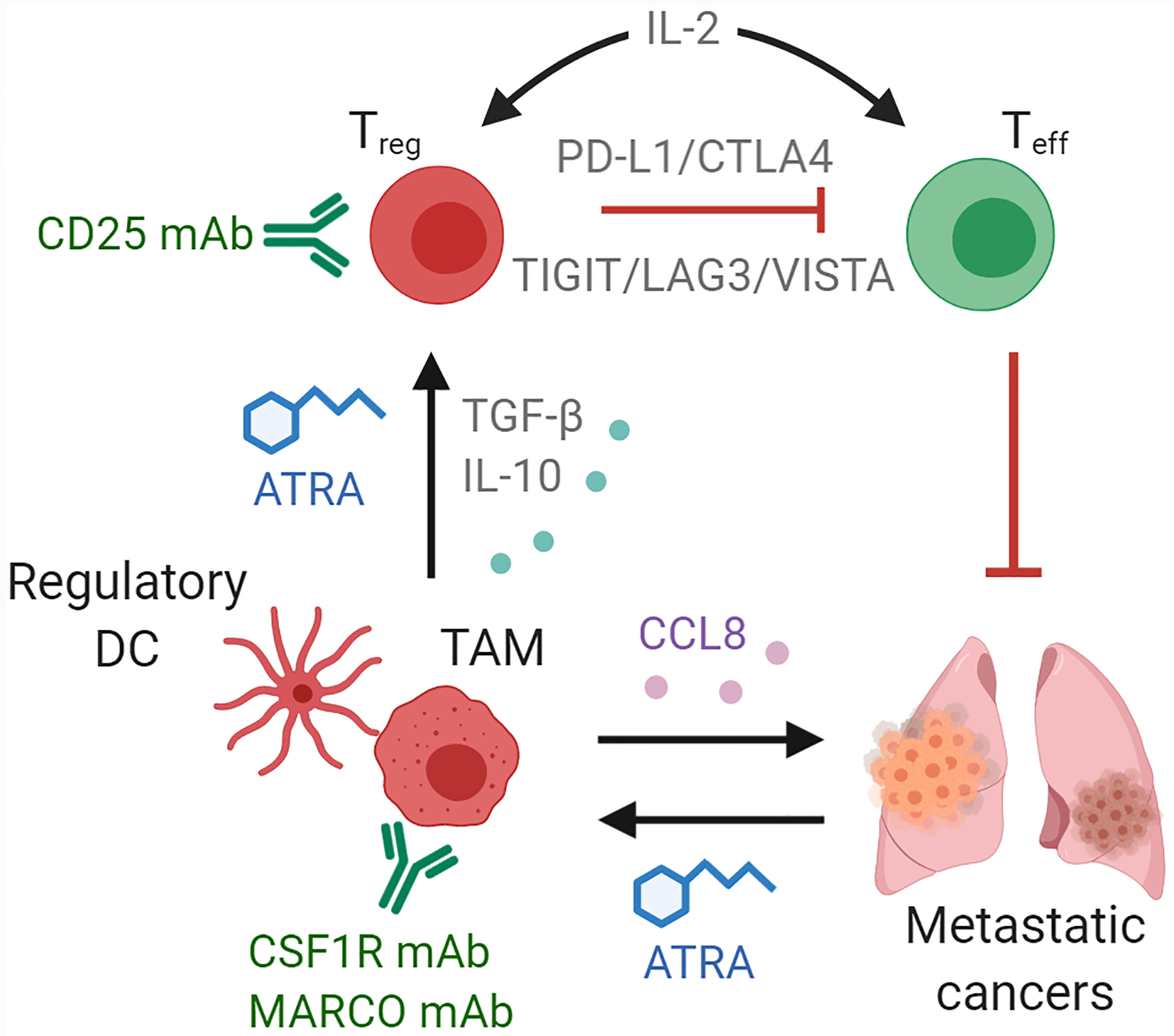
The systemic spread of tumor cells is the ultimate cause of the majority of deaths from cancer, yet few successful therapeutic strategies have emerged to specifically target metastasis. Here we discuss recent advances in our understanding of tumor-intrinsic pathways driving metastatic colonization and therapeutic resistance, as well as immune activating strategies to target metastatic disease. We focus on therapeutically exploitable mechanisms, promising strategies in preclinical and clinical development, and emerging areas with potential to become innovative treatments.
Conflict of interest statement
Conflicts of interest ME holds equity interest and a management position in KayoThera, a company developing cancer therapeutics. YK holds equity interest in KayoThera and Firebrand Therapeutics, and is a member of Scientific Advisory Boards of Kayothera, Firebrand Therapeutics, and Cytocares. YK has consulted for Merck, Amgen, Ono Pharma and has previously received funding support from Merck, Amgen, Johnson & Johnson, Janssen, Glycomimetics, and Ono Pharma. SG has consulted for Merck, Roche, Foundation Medicine, Foghorn Therapeutics, Novartis, Silagene, EQRX and Inspirata, has received research funding from M2GEN, and has equity interest in Inspirata and Silagene.
Figures
References
-
- Chaffer CL & Weinberg RA A perspective on cancer cell metastasis. Science 331, 1559–1564 (2011). - PubMed
-
- Siegel RL, Miller KD & Jemal A Cancer statistics, 2020. CA Cancer J Clin 70, 7–30 (2020). - PubMed
-
- Wei SC, Duffy CR & Allison JP Fundamental Mechanisms of Immune Checkpoint Blockade Therapy. Cancer Discov 8, 1069–1086 (2018). - PubMed
-
- Litwin MS & Tan HJ The Diagnosis and Treatment of Prostate Cancer: A Review. JAMA 317, 2532–2542 (2017). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
