

Abnormal Cardiac Repolarization After Seizure Episodes in Structural Brain Diseases: Cardiac Manifestation of Electrical Remodeling in the Brain?
- PMID: 33899505
- PMCID: PMC8200721
- DOI: 10.1161/JAHA.120.019778
Abnormal Cardiac Repolarization After Seizure Episodes in Structural Brain Diseases: Cardiac Manifestation of Electrical Remodeling in the Brain?
Abstract
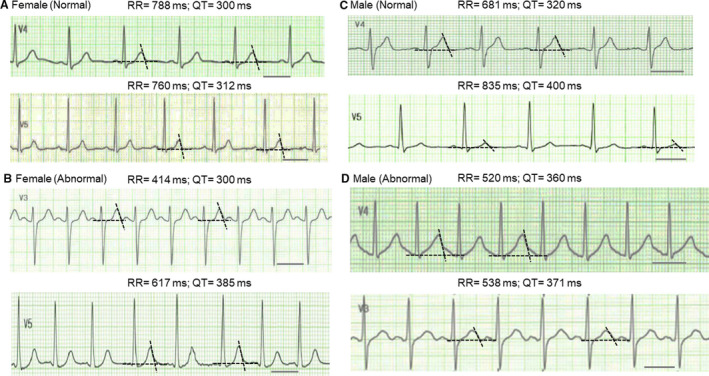
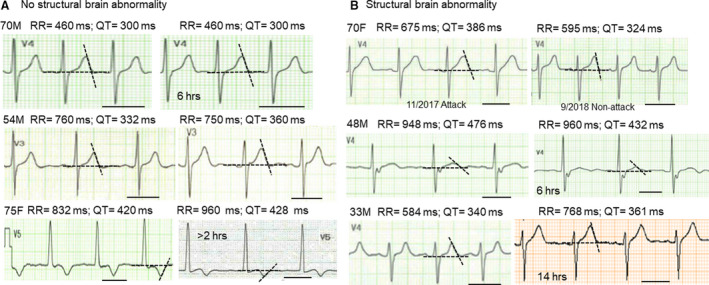
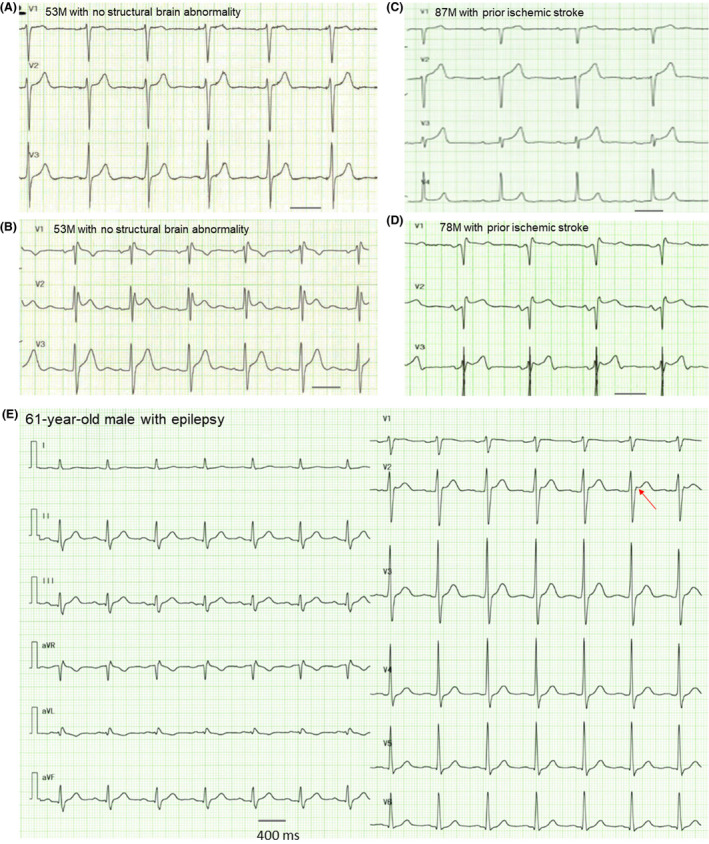
Background Abnormal cardiac repolarization is observed in patients with epilepsy and can be associated with sudden death. We investigated whether structural brain abnormalities are correlated with abnormal cardiac repolarizations in patients with seizure or epilepsy. Methods and Results We retrospectively analyzed and compared 12-lead ECG parameters following seizures between patients with and without structural brain abnormalities. A total of 96 patients were included: 33 women (17 with and 16 without brain abnormality) and 63 men (44 with and 19 without brain abnormality). Brain abnormalities included past stroke, chronic hematoma, remote bleeding, tumor, trauma, and postsurgical state. ECG parameters were comparable for heart rate, PR interval, and QRS duration between groups. In contrast, corrected QT intervals evaluated by Fridericia, Framingham, and Bazett formulas were prolonged in patients with brain abnormality compared with those without (women: Fridericia [normal versus abnormal], 397.4±32.7 versus 470.9±48.9; P=0.002; Framingham, 351.0±40.1 versus 406.2±46.1; P=0.002; Bazett, 423.8±38.3 versus 507.7±56.6; P<0.0001; men: Fridericia, 403.8±30.4 versus 471.0±47.1; P<0.0001; Framingham, 342.7±36.4 versus 409.4±45.8; P<0.0001; Bazett, 439.3±38.6 versus 506.2±56.8; P<0.0001). QT dispersion and Tpeak-Tend intervals were comparable between groups. We also observed abnormal ST-segment elevation in 5 patients. Importantly, no patients showed fatal arrhythmias during or after seizures. Conclusions Our study demonstrated that brain abnormalities can be associated with abnormal cardiac repolarization after seizures, which might be a manifestation of electrophysiological remodeling in the brain.
Keywords: QT prolongation; ST‐segment elevation; seizure; sudden death.
Conflict of interest statement
None.
Figures
Similar articles
-
Seizure-related cardiac repolarization abnormalities are associated with ictal hypoxemia.Epilepsia. 2011 Nov;52(11):2105-11. doi: 10.1111/j.1528-1167.2011.03262.x. Epub 2011 Sep 11. Epilepsia. 2011. PMID: 21906052 Free PMC article.
-
Interictal cardiac repolarization abnormalities in people with epilepsy.Epilepsy Behav. 2018 Feb;79:106-111. doi: 10.1016/j.yebeh.2017.10.028. Epub 2017 Dec 20. Epilepsy Behav. 2018. PMID: 29274604
-
Electrocardiographic conduction and repolarization markers associated with sudden cardiac death: moving along the electrocardiography waveform.Minerva Cardioangiol. 2019 Apr;67(2):131-144. doi: 10.23736/S0026-4725.18.04775-8. Epub 2018 Sep 26. Minerva Cardioangiol. 2019. PMID: 30260143 Review.
-
Tpeak-to-Tend/QT is an independent predictor of early ventricular arrhythmias and arrhythmic death in anterior ST elevation myocardial infarction patients.Eur Heart J Acute Cardiovasc Care. 2016 Oct;5(6):473-480. doi: 10.1177/2048872615598616. Epub 2015 Jul 30. Eur Heart J Acute Cardiovasc Care. 2016. PMID: 26228447
-
Traditional and novel electrocardiographic conduction and repolarization markers of sudden cardiac death.Europace. 2017 May 1;19(5):712-721. doi: 10.1093/europace/euw280. Europace. 2017. PMID: 27702850 Review.
Cited by
-
Electrocardiogram Changes in the Postictal Phase of Epileptic Seizure: Results from a Prospective Study.J Clin Med. 2023 Jun 17;12(12):4098. doi: 10.3390/jcm12124098. J Clin Med. 2023. PMID: 37373791 Free PMC article.
-
Manifested U-Waves Prior to Seizure Attacks in a Patient Who Had Remote Subarachnoid Hemorrhage: A Case Report.Ann Noninvasive Electrocardiol. 2024 Sep;29(5):e70014. doi: 10.1111/anec.70014. Ann Noninvasive Electrocardiol. 2024. PMID: 39297695 Free PMC article.
References
-
- Scheffer IE, Berkovic S, Capovilla G, Connolly MB, French J, Guilhoto L, Hirsch E, Jain S, Mathern GW, Moshé SL, et al. ILAE classification of the epilepsies: position paper of the ILAE Commission for Classification and Terminology. Epilepsia. 2017;58:512–521. DOI: 10.1111/epi.13709. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
