

Epidemiology of Cardiopulmonary Resuscitation in Critically Ill Children Admitted to Pediatric Intensive Care Units Across England: A Multicenter Retrospective Cohort Study
- PMID: 33899512
- PMCID: PMC8200770
- DOI: 10.1161/JAHA.120.018177
Epidemiology of Cardiopulmonary Resuscitation in Critically Ill Children Admitted to Pediatric Intensive Care Units Across England: A Multicenter Retrospective Cohort Study
Abstract
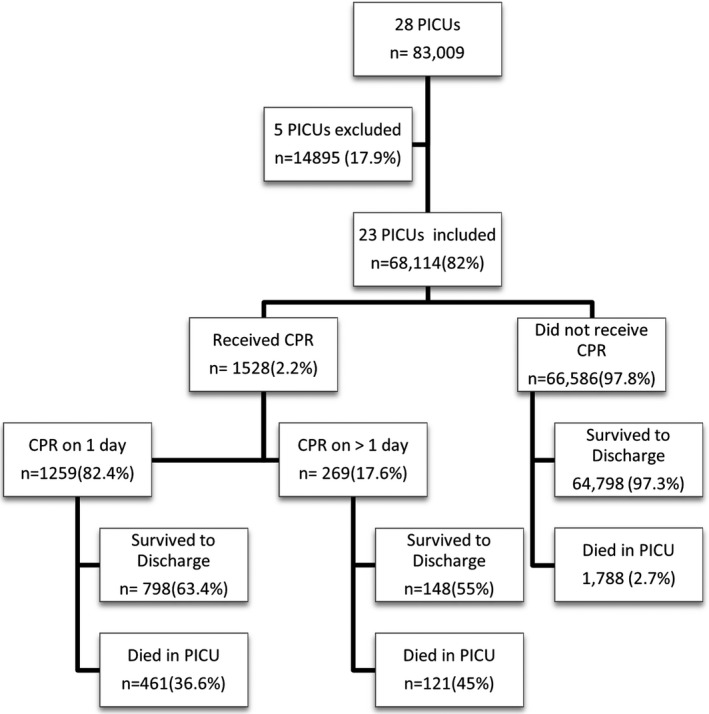
Background Cardiopulmonary arrests are a major contributor to mortality and morbidity in pediatric intensive care units (PICUs). Understanding the epidemiology and risk factors for CPR may inform national quality improvement initiatives. Methods and Results A retrospective cohort analysis using prospectively collected data from the Paediatric Intensive Care Audit Network database. The Paediatric Intensive Care Audit Network contains data on all PICU admissions in the United Kingdom. We identified children who received cardiopulmonary resuscitation (CPR) in 23 PICUs in England (2013-2017). Incidence rates of CPR and associated factors were analyzed. Logistic regression was used to estimate the size and precision of associations. Cumulative incidence of CPR was 2.2% for 68 114 admissions over 5 years with an incidence rate of 4.9 episodes/1000 bed days. Cardiovascular diagnosis (odds ratio [OR], 2.30; 95% CI, 2.02-2.61), age <1 year (OR, 1.84; 95% CI, 1.65-2.04), the Paediatric Index of Mortality 2 score on admission (OR, 1.045; 95% CI, 1.042-1.047) and longer length of stay (OR, 1.013; 95% CI, 1.012-1.014) were associated with increased odds of receiving CPR. We also found a higher risk of CPR associated with a history of preadmission cardiac arrest (OR, 20.69; [95% CI, 18.16-23.58) and for children with a cardiac condition admitted to a noncardiac PICU (OR, 2.75; 95% CI, 1.91-3.98). Children from Black (OR, 1.68; 95% CI, 1.36-2.07) and Asian (OR, 1.49; 95% CI, 1.28-1.74) racial/ethnic backgrounds were at higher risk of receiving CPR in PICU than White children. Conclusions Data from this first multicenter study from England provides a foundation for further research and evidence for benchmarking and quality improvement for prevention of cardiac arrests in PICU.
Keywords: cardiopulmonary resuscitation; critical care; outcome; pediatric; risk.
Conflict of interest statement
Dr Scholefield is funded by a National Institute for Health Research (Clinical Scientist) Fellowship award. However, this project was not funded by the National Institute for Health Research. The views expressed are those of the authors and not necessarily those of the NHS, the National Institute for Health Research, or the Department of Health and Social Care. The remaining authors have no disclosures to report.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
