

Bioengineering approaches to mature induced pluripotent stem cell-derived atrial cardiomyocytes to model atrial fibrillation
- PMID: 33899540
- PMCID: PMC8381703
- DOI: 10.1177/15353702211009146
Bioengineering approaches to mature induced pluripotent stem cell-derived atrial cardiomyocytes to model atrial fibrillation
Abstract
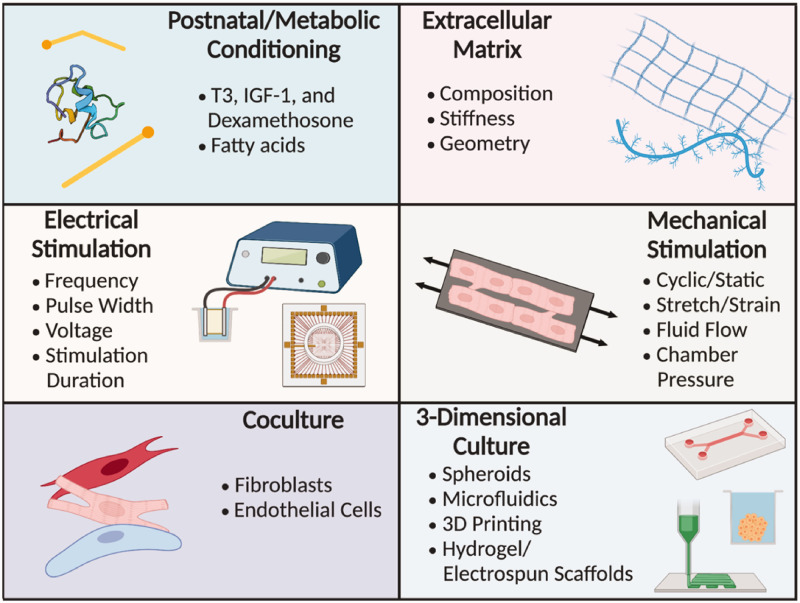
Induced pluripotent stem cells (iPSCs) serve as a robust platform to model several human arrhythmia syndromes including atrial fibrillation (AF). However, the structural, molecular, functional, and electrophysiological parameters of patient-specific iPSC-derived atrial cardiomyocytes (iPSC-aCMs) do not fully recapitulate the mature phenotype of their human adult counterparts. The use of physiologically inspired microenvironmental cues, such as postnatal factors, metabolic conditioning, extracellular matrix (ECM) modulation, electrical and mechanical stimulation, co-culture with non-parenchymal cells, and 3D culture techniques can help mimic natural atrial development and induce a more mature adult phenotype in iPSC-aCMs. Such advances will not only elucidate the underlying pathophysiological mechanisms of AF, but also identify and assess novel mechanism-based therapies towards supporting a more 'personalized' (i.e. patient-specific) approach to pharmacologic therapy of AF.
Keywords: Atrial fibrillation; disease modeling; human-induced pluripotent stem cell-derived atrial cardiomyocytes; maturation; pharmacologic response.
Conflict of interest statement
Figures
References
-
- Miyasaka Y, Barnes ME, Gersh BJ, Cha SS, Bailey KR, Abhayaratna WP, Seward JB, Tsang TSM. Secular trends in incidence of atrial fibrillation in Olmsted county, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation 2006; 114:119–25 - PubMed
-
- Lloyd-Jones DM, Wang TJ, Leip EP, Larson MG, Levy D, Vasan RS, D’Agostino RB, Massaro JM, Beiser A, Wolf PA, Benjamin EJ. Lifetime risk for development of atrial fibrillation: the Framingham heart study. Circulation 2004; 110:1042–6 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources