

Predictors of 30-Day Mortality Among Dutch Patients Undergoing Colorectal Cancer Surgery, 2011-2016
- PMID: 33900400
- PMCID: PMC8076964
- DOI: 10.1001/jamanetworkopen.2021.7737
Predictors of 30-Day Mortality Among Dutch Patients Undergoing Colorectal Cancer Surgery, 2011-2016
Erratum in
-
Error in Byline.JAMA Netw Open. 2021 Aug 2;4(8):e2127694. doi: 10.1001/jamanetworkopen.2021.27694. JAMA Netw Open. 2021. PMID: 34410401 Free PMC article. No abstract available.
Abstract
Importance: Quality improvement programs for colorectal cancer surgery have been introduced with benchmarking based on quality indicators, such as mortality. Detailed (pre)operative characteristics may offer relevant information for proper case-mix correction.
Objective: To investigate the added value of machine learning to predict quality indicators for colorectal cancer surgery and identify previously unrecognized predictors of 30-day mortality based on a large, nationwide colorectal cancer registry that collected extensive data on comorbidities.
Design, setting, and participants: All patients who underwent resection for primary colorectal cancer registered in the Dutch ColoRectal Audit between January 1, 2011, and December 31, 2016, were included. Multiple machine learning models (multivariable logistic regression, elastic net regression, support vector machine, random forest, and gradient boosting) were made to predict quality indicators. Model performance was compared with conventionally used scores. Risk factors were identified by logistic regression analyses and Shapley additive explanations (ie, SHAP values). Statistical analysis was performed between March 1 and September 30, 2020.
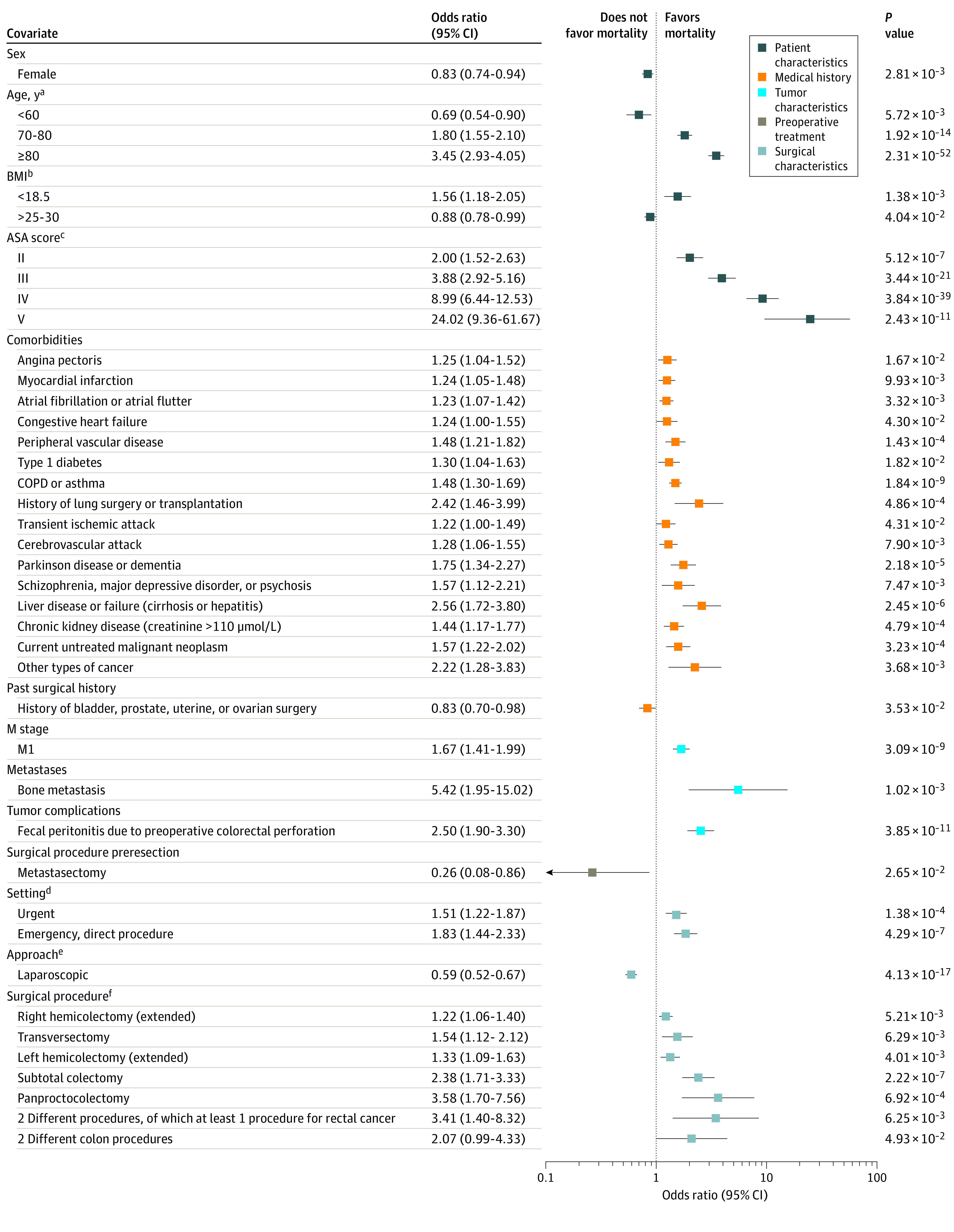
Main outcomes and measures: The primary outcome of this cohort study was 30-day mortality. Prediction models were trained on a training set by performing 5-fold cross-validation, and outcomes were measured by the area under the receiver operating characteristic curve on the test set. Machine learning was further used to identify risk factors, measured by odds ratios and SHAP values.
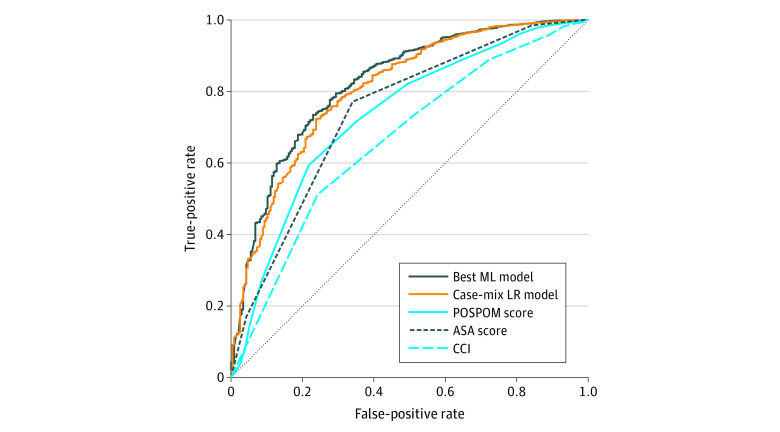
Results: This cohort study included 62 501 records, most patients were male (35 116 [56.2%]), were aged 61 to 80 years (41 560 [66.5%]), and had an American Society of Anesthesiology score of II (35 679 [57.1%]). A 30-day mortality rate of 2.7% (n = 1693) was found. The area under the curve of the best machine learning model for 30-day mortality (0.82; 95% CI, 0.79-0.85) was significantly higher than the American Society of Anesthesiology score (0.74; 95% CI, 0.71-0.77; P < .001), Charlson Comorbidity Index (0.66; 95% CI, 0.63-0.70; P < .001), and preoperative score to predict postoperative mortality (0.73; 95% CI, 0.70-0.77; P < .001). Hypertension, myocardial infarction, chronic obstructive pulmonary disease, and asthma were comorbidities with a high risk for increased mortality. Machine learning identified specific risk factors for a complicated course, intensive care unit admission, prolonged hospital stay, and readmission. Laparoscopic surgery was associated with a decreased risk for all adverse outcomes.
Conclusions and relevance: This study found that machine learning methods outperformed conventional scores to predict 30-day mortality after colorectal cancer surgery, identified specific patient groups at risk for adverse outcomes, and provided directions to optimize benchmarking in clinical audits.
Conflict of interest statement
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
