

Sustained oxygenation improvement after first prone positioning is associated with liberation from mechanical ventilation and mortality in critically ill COVID-19 patients: a cohort study
- PMID: 33900484
- PMCID: PMC8072095
- DOI: 10.1186/s13613-021-00853-1
Sustained oxygenation improvement after first prone positioning is associated with liberation from mechanical ventilation and mortality in critically ill COVID-19 patients: a cohort study
Abstract
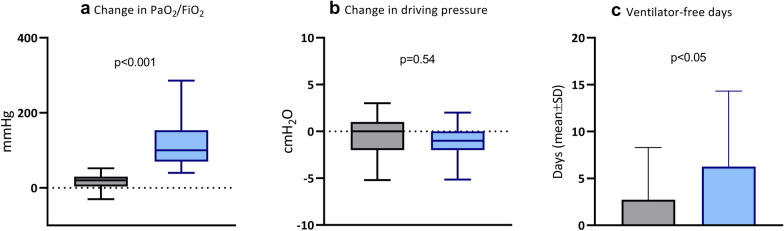
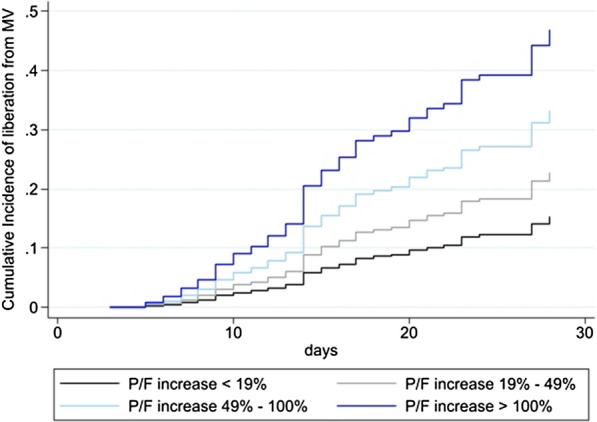
Background: Prone positioning (PP) has been used to improve oxygenation in patients affected by the SARS-CoV-2 disease (COVID-19). Several mechanisms, including lung recruitment and better lung ventilation/perfusion matching, make a relevant rational for using PP. However, not all patients maintain the oxygenation improvement after returning to supine position. Nevertheless, no evidence exists that a sustained oxygenation response after PP is associated to outcome in mechanically ventilated COVID-19 patients. We analyzed data from 191 patients affected by COVID-19-related acute respiratory distress syndrome undergoing PP for clinical reasons. Clinical history, severity scores and respiratory mechanics were analyzed. Patients were classified as responders (≥ median PaO2/FiO2 variation) or non-responders (< median PaO2/FiO2 variation) based on the PaO2/FiO2 percentage change between pre-proning and 1 to 3 h after re-supination in the first prone positioning session. Differences among the groups in physiological variables, complication rates and outcome were evaluated. A competing risk regression analysis was conducted to evaluate if PaO2/FiO2 response after the first pronation cycle was associated to liberation from mechanical ventilation.
Results: The median PaO2/FiO2 variation after the first PP cycle was 49 [19-100%] and no differences were found in demographics, comorbidities, ventilatory treatment and PaO2/FiO2 before PP between responders (96/191) and non-responders (95/191). Despite no differences in ICU length of stay, non-responders had a higher rate of tracheostomy (70.5% vs 47.9, P = 0.008) and mortality (53.7% vs 33.3%, P = 0.006), as compared to responders. Moreover, oxygenation response after the first PP was independently associated to liberation from mechanical ventilation at 28 days and was increasingly higher being higher the oxygenation response to PP.
Conclusions: Sustained oxygenation improvement after first PP session is independently associated to improved survival and reduced duration of mechanical ventilation in critically ill COVID-19 patients.
Keywords: COVID19; ICU; Prone positioning; Ventilatory free days.
Conflict of interest statement
GS received a grant from the Italian society of anesthesia (SIAARTI) and a travel grant from PLUG group (ESICM 2019) not related to the current analysis.
Figures
References
-
- COVID-19 Map. Johns Hopkins Coronavirus. Resour Cent. 2021. https://coronavirus.jhu.edu/map.html. Accessed 7 Apr 2021.
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
