

Ground-glass opacity (GGO): a review of the differential diagnosis in the era of COVID-19
- PMID: 33900542
- PMCID: PMC8071755
- DOI: 10.1007/s11604-021-01120-w
Ground-glass opacity (GGO): a review of the differential diagnosis in the era of COVID-19
Abstract
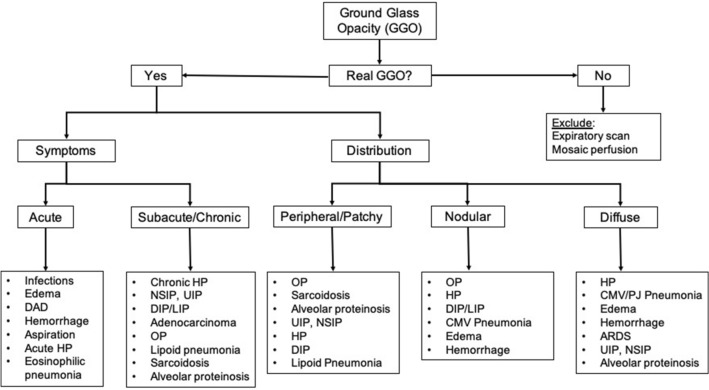
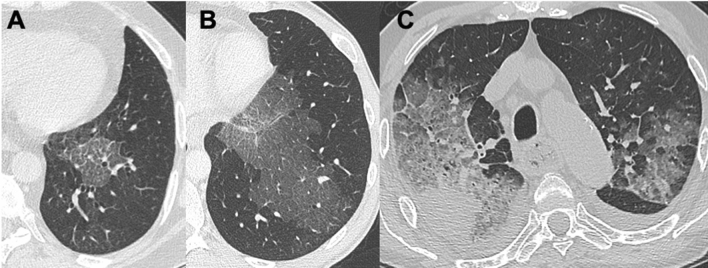
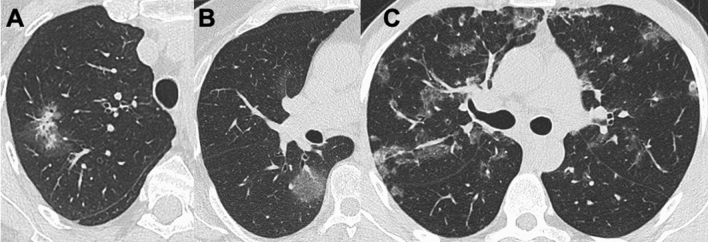
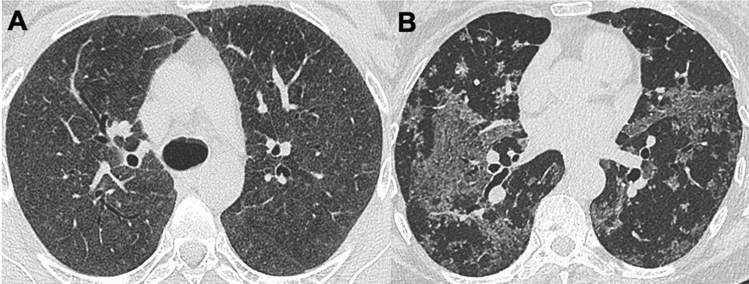
Thoracic imaging is fundamental in the diagnostic route of Coronavirus disease 2019 (COVID-19) especially in patients admitted to hospitals. In particular, chest computed tomography (CT) has a key role in identifying the typical features of the infection. Ground-glass opacities (GGO) are one of the main CT findings, but their presence is not specific for this viral pneumonia. In fact, GGO is a radiological sign of different pathologies with both acute and subacute/chronic clinical manifestations. In the evaluation of a subject with focal or diffuse GGO, the radiologist has to know the patient's medical history to obtain a valid diagnostic hypothesis. The authors describe the various CT appearance of GGO, related to the onset of symptoms, focusing also on the ancillary signs that can help radiologist to obtain a correct and prompt diagnosis.
Keywords: COVID-19; Computed tomography; Coronavirus; Differential diagnosis; Ground-glass opacity.
© 2021. Japan Radiological Society.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

Similar articles
-
COVID-19 pneumonia: CT findings of 122 patients and differentiation from influenza pneumonia.Eur Radiol. 2020 Oct;30(10):5463-5469. doi: 10.1007/s00330-020-06928-0. Epub 2020 May 12. Eur Radiol. 2020. PMID: 32399710 Free PMC article.
-
Artificial intelligence-based analysis of the spatial distribution of abnormal computed tomography patterns in SARS-CoV-2 pneumonia: association with disease severity.Respir Res. 2024 Jan 10;25(1):24. doi: 10.1186/s12931-024-02673-w. Respir Res. 2024. PMID: 38200566 Free PMC article.
-
Pitfalls of Computed Tomography in the Coronavirus 2019 (COVID-19) Era: A New Perspective on Ground-Glass Opacities.Cureus. 2020 May 16;12(5):e8151. doi: 10.7759/cureus.8151. Cureus. 2020. PMID: 32550070 Free PMC article.
-
Comparison of the computed tomography findings in COVID-19 and other viral pneumonia in immunocompetent adults: a systematic review and meta-analysis.Eur Radiol. 2020 Dec;30(12):6485-6496. doi: 10.1007/s00330-020-07018-x. Epub 2020 Jun 27. Eur Radiol. 2020. PMID: 32594211 Free PMC article.
-
Diagnostic accuracy of CT and radiographic findings for novel coronavirus 2019 pneumonia: Systematic review and meta-analysis.Clin Imaging. 2021 Apr;72:75-82. doi: 10.1016/j.clinimag.2020.11.021. Epub 2020 Nov 11. Clin Imaging. 2021. PMID: 33217674 Free PMC article.
Cited by
-
How accurate is high-resolution computed tomography of the chest in differentiating between pulmonary invasive fungal infections and other pulmonary infections in children with cancer?Pediatr Radiol. 2025 Feb;55(2):268-279. doi: 10.1007/s00247-024-06112-2. Epub 2024 Dec 17. Pediatr Radiol. 2025. PMID: 39688678
-
EffViT-COVID: A dual-path network for COVID-19 percentage estimation.Expert Syst Appl. 2023 Mar 1;213:118939. doi: 10.1016/j.eswa.2022.118939. Epub 2022 Oct 3. Expert Syst Appl. 2023. PMID: 36210962 Free PMC article.
-
COVLIAS 3.0: cloud-based quantized hybrid UNet3+ deep learning for COVID-19 lesion detection in lung computed tomography.Front Artif Intell. 2024 Jun 28;7:1304483. doi: 10.3389/frai.2024.1304483. eCollection 2024. Front Artif Intell. 2024. PMID: 39006802 Free PMC article.
-
Imaging of metabolic and overload disorders in tissues and organs.Jpn J Radiol. 2023 Jun;41(6):571-595. doi: 10.1007/s11604-022-01379-7. Epub 2023 Jan 21. Jpn J Radiol. 2023. PMID: 36680702 Review.
-
[Diagnostic protocol for febrile lung infiltrates during the COVID-19 pandemic].Medicine (Madr). 2022 May;13(55):3261-3265. doi: 10.1016/j.med.2022.05.009. Epub 2022 May 12. Medicine (Madr). 2022. PMID: 35582697 Free PMC article. Spanish.
References
-
- Agostini A, Floridi C, Borgheresi A, et al. Proposal of a low-dose, long-pitch, dual-source chest CT protocol on third-generation dual source CT using a tin filter for spectral shaping at 100kVp for coronavirus disease 2019 (COVID-19) patients: a feasibility study. Radiol Med (Torino) 2020;125(4):365–373. doi: 10.1007/s11547-020-01179-x. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
