

Characteristics and Clinical Implications of Carbapenemase-Producing Klebsiella pneumoniae Colonization and Infection, Italy
- PMID: 33900910
- PMCID: PMC8084501
- DOI: 10.3201/eid2705.203662
Characteristics and Clinical Implications of Carbapenemase-Producing Klebsiella pneumoniae Colonization and Infection, Italy
Abstract
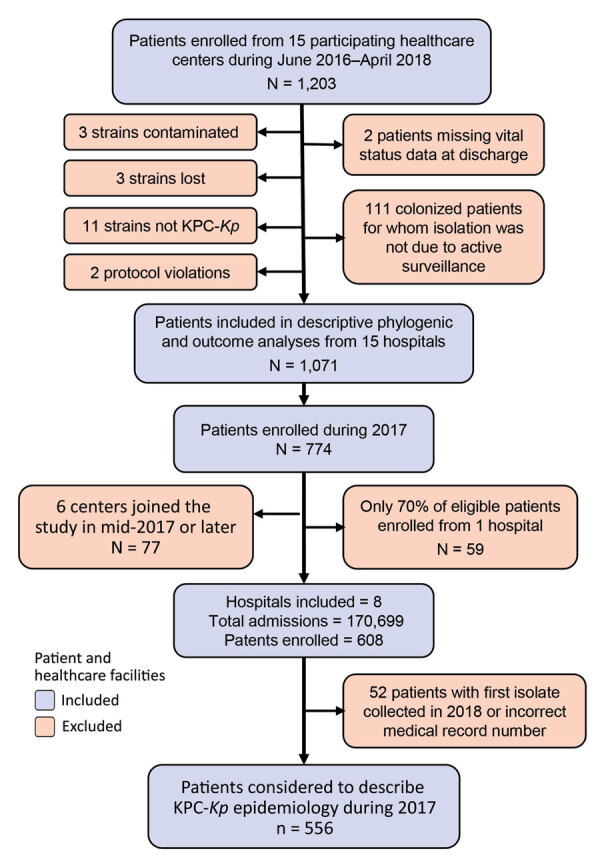
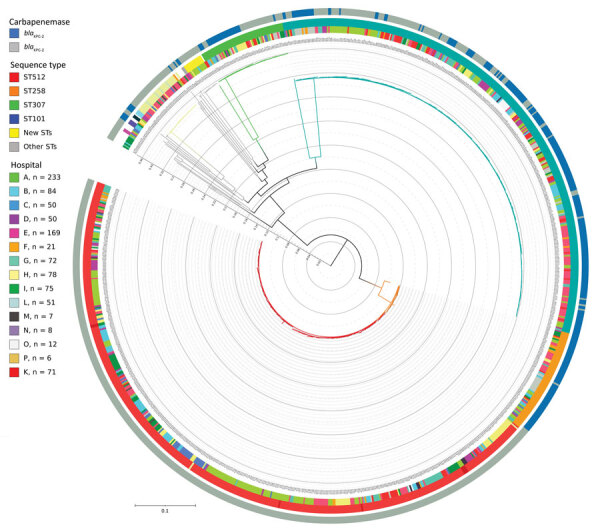
Klebsiella pneumoniae carbapenemase–producing K. pneumoniae (KPC-Kp) has been endemic in Italy since 2013. In a multicenter cohort study, we investigated various aspects of KPC-Kp among patients, including 15-day mortality rates and delays in adequate therapy. Most (77%) KPC-Kp strains were sequence type (ST) ST512 or ST307. During 2017, KPC-Kp prevalence was 3.26 cases/1,000 hospitalized patients. Cumulative incidence of KPC-Kp acquired >48 hours after hospital admission was 0.68% but varied widely between centers. Among patients with mild infections and noninfected colonized patients, 15-day mortality rates were comparable, but rates were much higher among patients with severe infections. Delays of
Keywords: CRE; Carbapenem resistance; Enterobacteriaceae; Italy; KPC-Kp; Klebsiella pneumoniae; antimicrobial resistance; bacteria; healthcare-associated infections; mortality rates.
Figures
References
-
- Tumbarello M, Viale P, Viscoli C, Trecarichi EM, Tumietto F, Marchese A, et al. Predictors of mortality in bloodstream infections caused by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae: importance of combination therapy. Clin Infect Dis. 2012;55:943–50. 10.1093/cid/cis588 - DOI - PubMed
-
- Stewardson AJ, Marimuthu K, Sengupta S, Allignol A, El-Bouseary M, Carvalho MJ, et al. Effect of carbapenem resistance on outcomes of bloodstream infection caused by Enterobacteriaceae in low-income and middle-income countries (PANORAMA): a multinational prospective cohort study. Lancet Infect Dis. 2019;19:601–10. 10.1016/S1473-3099(18)30792-8 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
