

Determination of Work Relative Value Units for Management of Lumbar Spinal Stenosis by Open Decompression and Interlaminar Stabilization
- PMID: 33900951
- PMCID: PMC7931742
- DOI: 10.14444/8026
Determination of Work Relative Value Units for Management of Lumbar Spinal Stenosis by Open Decompression and Interlaminar Stabilization
Abstract
Background: Effective January 1, 2017, open surgical decompression and interlaminar stabilization (ILS) received a Category I Current Procedural Terminology (CPT®) code 22867. The current work relative value units (wRVUs) assigned to the procedure of 13.5 are not reflective of the amount of work involved. During the survey process, CPT® 22867 was erroneously assessed with a percutaneous "sister" code (CPT® 22869), which is performed with no decompression (but within the same new "family") and primarily by nonsurgeons. However, similar CPT® code descriptors assigned to each of these new codes undermined their procedural differences during the survey process and generated confusion among physician survey responders, the American Medical Association/Specialty Society Relative Value Scale Update Committee (RUC), and ultimately the Centers for Medicare and Medicaid Services (CMS) regarding the value of ILS. The resulting physician payment determination for the ILS procedure has had severe deleterious effects on this procedure being offered to lumbar spinal stenosis (LSS) patients. Our independent society-driven survey presents new data that assess the accuracy of the assigned wRVUs for CPT® 22867.
Methods: An independent survey was driven by the International Society for the Advancement of Spine Surgery (ISASS) in November 2018 and sent to 58 US surgeons with experience performing open decompression with ILS (CPT® 22867) and without financial conflicts of interest as analogous to RUC survey financial disclosure requests. Respondents were asked to compare CPT® 22867 with a list of 10 other comparator CPT® codes reflective of common spine surgeries. The survey presented each comparator CPT® code with its code descriptor and corresponding wRVUs alongside the code descriptor for CPT® 22867. A patient vignette was also provided that describes a typical clinical scenario for the surveyed procedure. Respondents were then asked to indicate which comparator CPT® code on the reference list is most similar to the survey code descriptor and typical patient/service vignette provided, as well as specify estimated wRVUs for CPT® 22867 relative to their selected comparator CPT® code. The surgeons' responses were analyzed to determine comparator CPT® codes and estimated wRVUs.
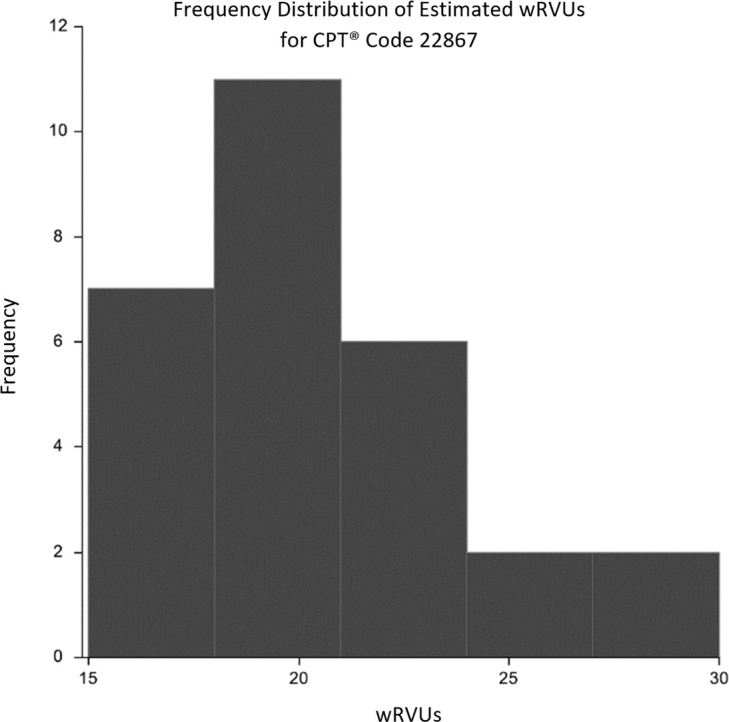
Results: Among the 28 surgeons who responded to the survey, both open decompression codes (57.1%) and fusion codes (42.9%) were chosen as most similar to the typical patient/service for CPT® 22867. Furthermore, the laminectomy procedure (CPT® 63047) was chosen as the surveyed surgeons' model response for a reference procedure in terms of similar work intensity and time for CPT® 22867. After calculating the difference between the selected comparator codes and estimated wRVUs, nearly all respondents had a positive calculated difference, indicating that surgeons selected wRVUs lower than they deemed appropriate as a result of the listed CPT® codes they were required to use. In the spirit of the Rasch analysis, the regression analysis estimated wRVUs for CPT® 22867 that are greater than its assigned wRVUs (13.5) and its most comparable procedure (CPT® 63047; reference wRVUs: 15.37).
Discussion and conclusions: The survey results indicate that the wRVUs assigned to CPT® 22867 are significantly undervalued at 13.50 and have directly resulted in the underreimbursement for surgeons performing the ILS procedure. This misvaluation of the code has created a supply-and-demand anomaly in which the rate of ILS procedures has flatlined despite increasing rates of fusion procedures and an increasing older population. This anomaly is a cause of concern for policy makers and the health care community for the future of safeguarding patient welfare and procedural innovation. Therefore, understanding the clinical economic impact and appropriately addressing potential misvalued codes, such as the ILS procedure, are critical to protecting the future of patient care.
Keywords: CPT® 22867; current procedural terminology (CPT®); decompression; interlaminar stabilization (ILS); lumbar spinal stenosis (LSS); physician payment; relative value units (RVUs).
This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2021 ISASS.
Conflict of interest statement
Figures




References
LinkOut - more resources
Full Text Sources
Other Literature Sources