

Augmented Reality Navigated Sacral-Alar-Iliac Screw Insertion
- PMID: 33900970
- PMCID: PMC7931709
- DOI: 10.14444/8021
Augmented Reality Navigated Sacral-Alar-Iliac Screw Insertion
Abstract
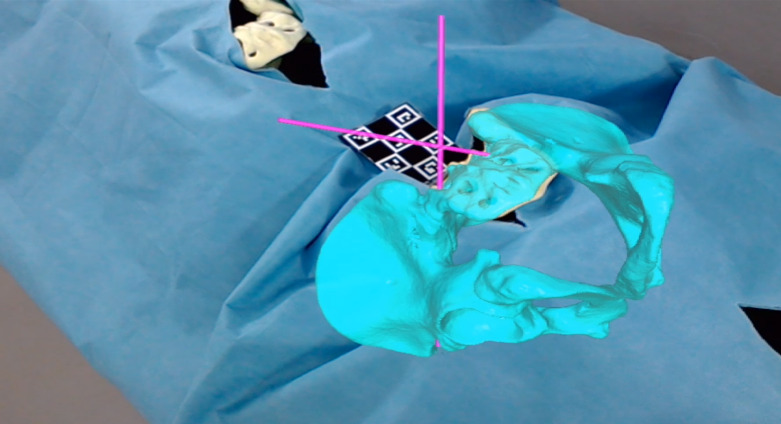
Background: Sacral-alar-iliac (SAI) screws are increasingly used for lumbo-pelvic fixation procedures. Insertion of SAI screws is technically challenging, and surgeons often rely on costly and time-consuming navigation systems. We investigated the accuracy and precision of an augmented reality (AR)-based and commercially available head-mounted device requiring minimal infrastructure.
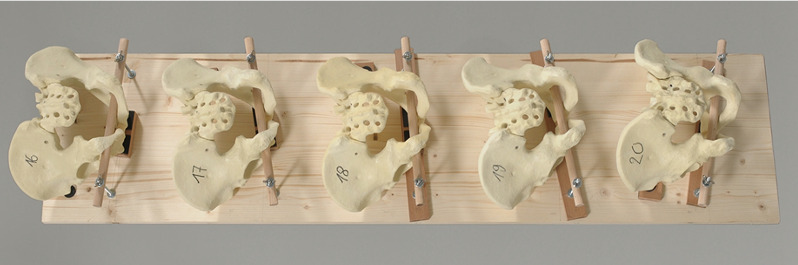
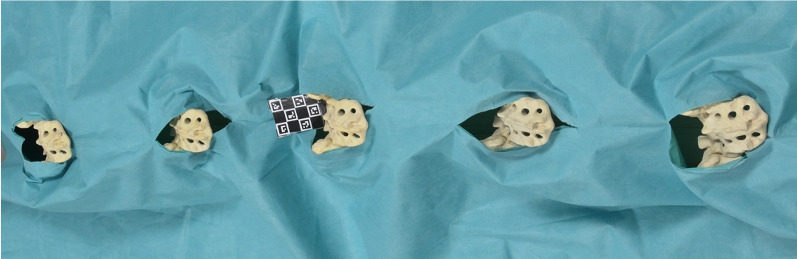
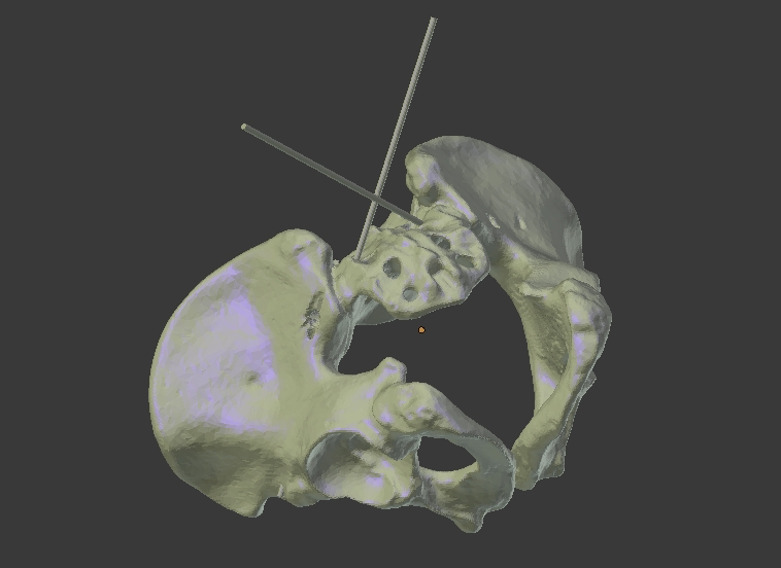
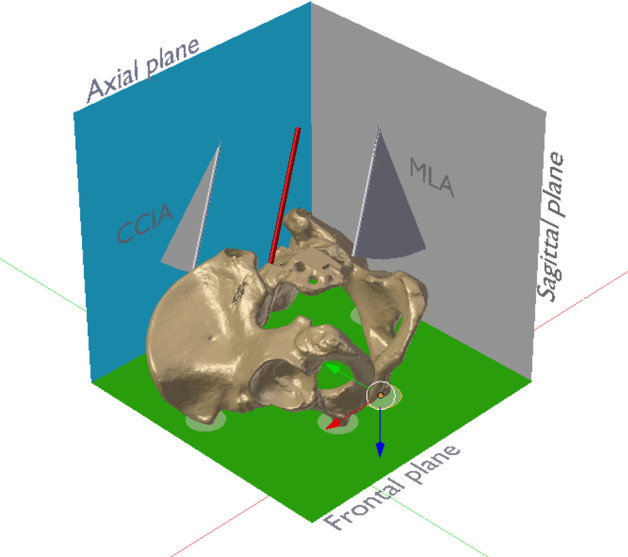
Methods: A pelvic sawbone model served to drill pilot holes of 80 SAI screw trajectories by 2 surgeons, randomly either freehand (FH) without any kind of navigation or with AR navigation. The number of primary pilot hole perforations, simulated screw perforation, minimal axis/outer cortical wall distance, true sagittal cranio-caudal inclination angle (tSCCIA), true axial medio-lateral angle, and maximal screw length (MSL) were measured and compared to predefined optimal values.
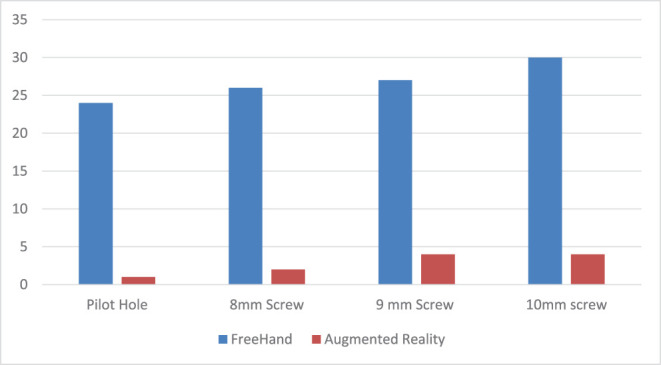
Results: In total, 1/40 (2.5%) of AR-navigated screw hole trajectories showed a perforation before passing the inferior gluteal line compared to 24/40 (60%) of FH screw hole trajectories (P < .05). The differences between FH- and AR-guided holes compared to optimal values were significant for tSCCIA with -10.8° ± 11.77° and MSL -65.29 ± 15 mm vs 55.04 ± 6.76 mm (P = .001).
Conclusions: In this study, the additional anatomical information provided by the AR headset and the superimposed operative plan improved the precision of drilling pilot holes for SAI screws in a laboratory setting compared to the conventional FH technique. Further technical development and validation studies are currently being performed to investigate potential clinical benefits of the AR-based navigation approach described here.
Level of evidence: 4.
Keywords: HoloLens; augmented reality; lumbo-pelvic fixation; mixed reality; navigation; sacral-alar-iliac.
This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2021 ISASS.
Conflict of interest statement
Figures


References
-
- Kebaish KM. Sacropelvic fixation: techniques and complications. Spine (Phila Pa 1976) 2010;35(25):2245–2251. - PubMed
-
- Bernhardt M, Swartz DE, Clothiaux PL, Crowell RR, White AA. Posterolateral lumbar and lumbosacral fusion with and without pedicle screw internal fixation. Clin Orthop Relat Res. 1992;(284):109–115. - PubMed
-
- Allen BL, Ferguson RL. The Galveston technique of pelvic fixation with L-rod instrumentation of the spine. Spine (Phila Pa 1976) 1984;9(4):388–394. - PubMed
-
- Molinari RW, Bridwell KH, Lenke LG, Ungacta FF, Riew KD. Complications in the surgical treatment of pediatric high-grade, isthmic dysplastic spondylolisthesis. A comparison of three surgical approaches. Spine (Phila Pa 1976) 1999;24(16):1701–1711. - PubMed
-
- Grubb SA, Lipscomb HJ. Results of lumbosacral fusion for degenerative disc disease with and without instrumentation. Two- to five-year follow-up. Spine (Phila Pa 1976) 1992;17(3):349–355. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous