

Staying on target: Maintaining a balanced resuscitation during damage-control resuscitation improves survival
- PMID: 33901052
- PMCID: PMC8547746
- DOI: 10.1097/TA.0000000000003245
Staying on target: Maintaining a balanced resuscitation during damage-control resuscitation improves survival
Abstract
Background: Damage-control resuscitation (DCR) improves survival in severely bleeding patients. However, deviating from balanced transfusion ratios during a resuscitation may limit this benefit. We hypothesized that maintaining a balanced resuscitation during DCR is independently associated with improved survival.
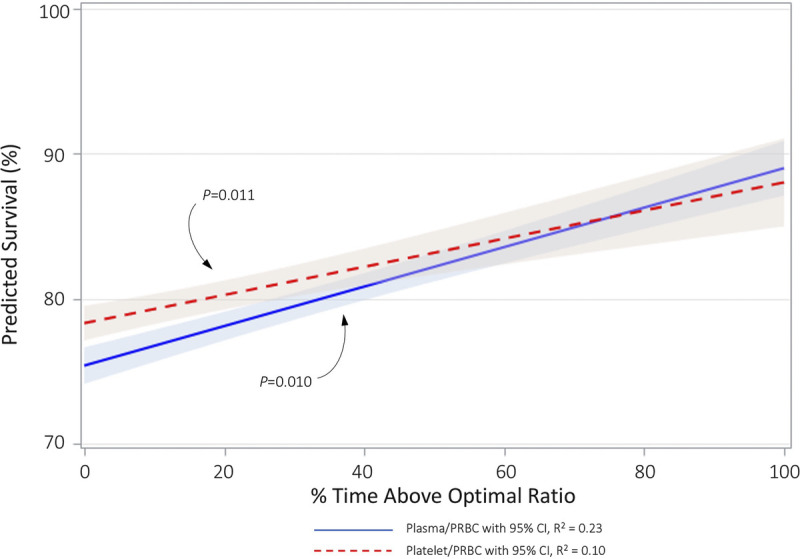
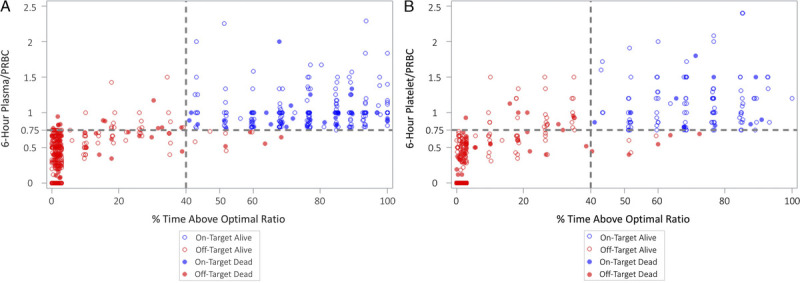
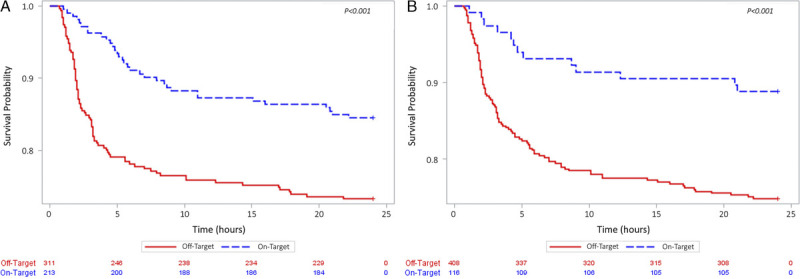
Methods: This was a secondary analysis of the Prospective Observational Multicenter Major Trauma Transfusion (PROMMTT) study. Patients receiving >3 U of packed red blood cells (PRBCs) during any 1-hour period over the first 6 hours and surviving beyond 30 minutes were included. Linear regression assessed the effect of percent time in a high-ratio range on 24-hour survival. We identified an optimal ratio and percent of time above the target ratio threshold by Youden's index. We compared patients with a 6-hour ratio above the target and above the percent time threshold (on-target) with all others (off-target). Kaplan-Meier analysis assessed the combined effect of blood product ratio and percent time over the target ratio on 24-hour and 30-day survival. Multivariable logistic regression identified factors independently associated with 24-hour and 30-day survival.
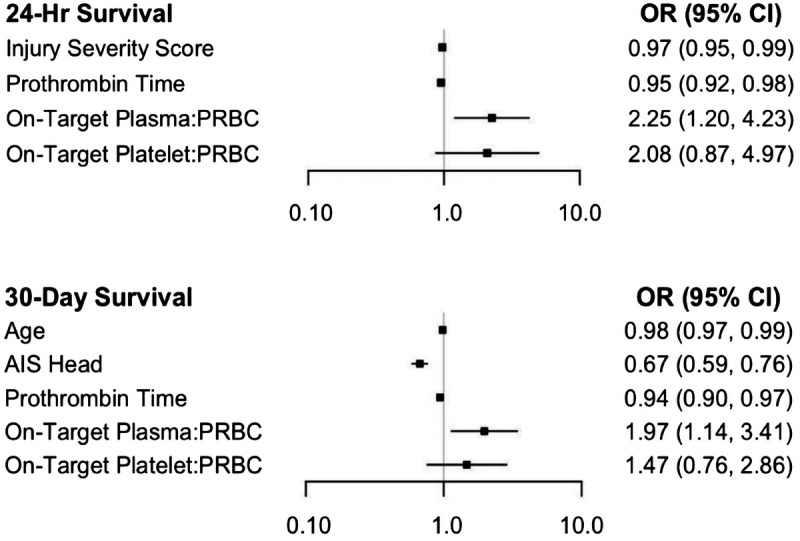
Results: Of 1,245 PROMMTT patients, 524 met the inclusion criteria. Optimal targets were plasma/PRBC and platelet/PRBC of 0.75 (3:4) and ≥40% time spent over this threshold. For plasma/PRBC, on-target (n = 213) versus off-target (n = 311) patients were younger (median, 31 years; interquartile range, [22-50] vs. 40 [25-54]; p = 0.002) with similar injury burdens and presenting physiology. Similar patterns were observed for platelet/PRBC on-target (n = 116) and off-target (n = 408) patients. After adjusting for differences, on-target plasma/PRBC patients had significantly improved 24-hour (odds ratio, 2.25; 95% confidence interval, 1.20-4.23) and 30-day (odds ratio, 1.97; 95% confidence interval, 1.14-3.41) survival, while on-target platelet/PRBC patients did not.
Conclusion: Maintaining a high ratio of plasma/PRBC during DCR is independently associated with improved survival. Performance improvement efforts and prospective studies should capture time spent in a high-ratio range.
Level of evidence: Epidemiologic/prognostic study, level II; Therapeutic, level IV.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Association for the Surgery of Trauma.
Figures
References
-
- Rhee P, Joseph B, Pandit V, Aziz H, Vercruysse G, Kulvatunyou N, Friese RS. Increasing trauma deaths in the United States. Ann Surg. 2014;260(1):13–21. - PubMed
-
- Cannon JW. Hemorrhagic shock. N Engl J Med. 2018;378(4):370–379. - PubMed
-
- Berwick D, Downey A, Cornett E. A National Trauma Care System: Integrating Military and Civilian Trauma Systems to Achieve Zero Preventable Deaths after Injury. Washington, DC: National Academies Press; 2016. - PubMed
-
- Eastridge BJ Hardin M Cantrell J, et al. Died of wounds on the battlefield: Causation and implications for improving combat casualty care. J Trauma. 2011;71(Suppl 1):S4–S8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
