

Estimating and characterizing the burden of multimorbidity in the community: A comprehensive multistep analysis of two large nationwide representative surveys in France
- PMID: 33901171
- PMCID: PMC8109815
- DOI: 10.1371/journal.pmed.1003584
Estimating and characterizing the burden of multimorbidity in the community: A comprehensive multistep analysis of two large nationwide representative surveys in France
Abstract
Background: Given the increasing burden of chronic conditions, multimorbidity is now a priority for healthcare and public health systems worldwide. Appropriate methodological approaches for assessing the phenomenon have not yet been established, resulting in inconsistent and incomplete descriptions. We aimed to estimate and characterize the burden of multimorbidity in the adult population in France in terms of number and type of conditions, type of underlying mechanisms, and analysis of the joint effects for identifying combinations with the most deleterious interaction effects on health status.
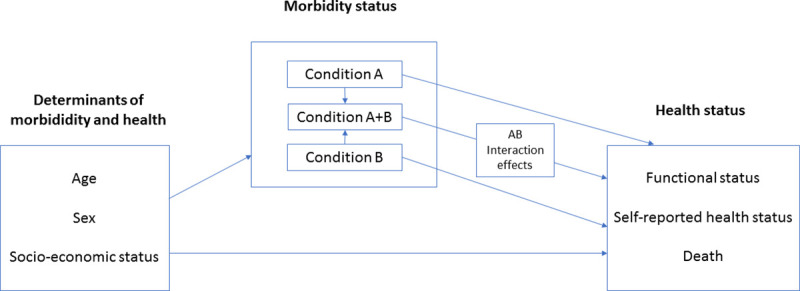
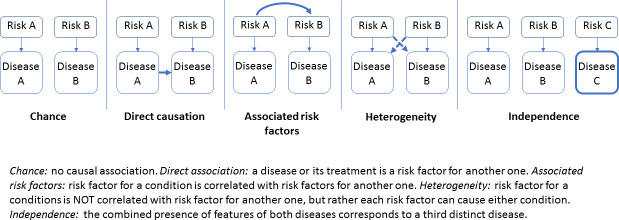
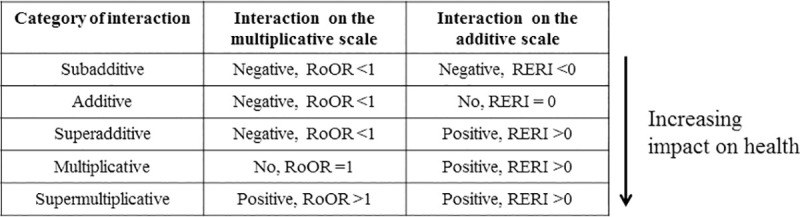
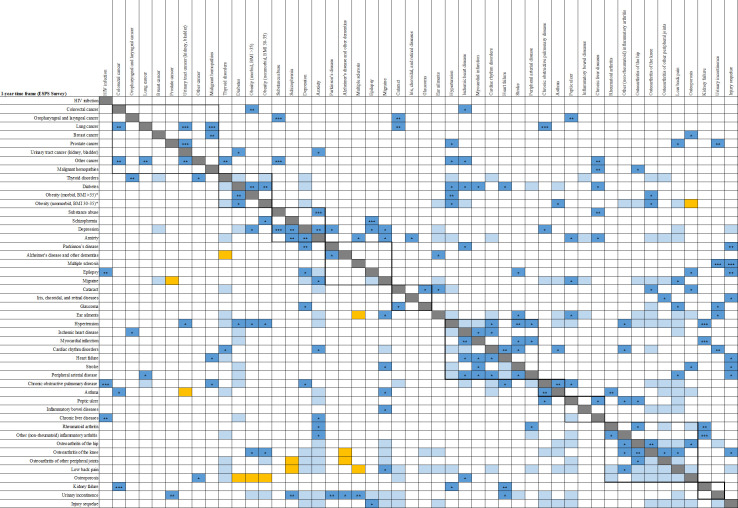
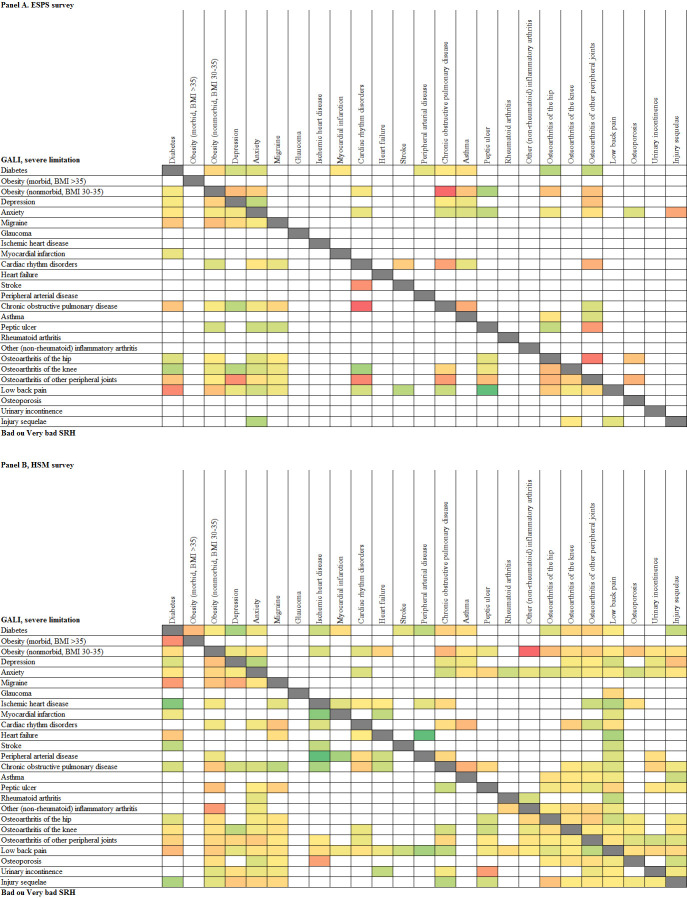
Methods and findings: We used a multistep approach to analyze cross-sectional and longitudinal data from 2 large nationwide representative surveys: 2010/2014 waves of the Health, Health Care, and Insurance Survey (ESPS 2010-2014) and Disability Healthcare Household Survey 2008 (HSM 2008), that collected similar data on 61 chronic or recurrent conditions. Adults aged ≥25 years in either ESPS 2010 (14,875) or HSM 2008 (23,348) were considered (participation rates were 65% and 62%, respectively). Longitudinal analyses included 7,438 participants of ESPS 2010 with follow-up for mortality (97%) of whom 3,798 were reinterviewed in 2014 (52%). Mortality, activity limitation, self-reported health, difficulties in activities/instrumental activities of daily living, and Medical Outcomes Study Short-Form 12-Item Health Survey were the health status measures. Multiple regression models were used to estimate the impact of chronic or recurrent conditions and multimorbid associations (dyads, triads, and tetrads) on health status. Etiological pathways explaining associations were investigated, and joint effects and interactions between conditions on health status measures were evaluated using both additive and multiplicative scales. Forty-eight chronic or recurrent conditions had an independent impact on mortality, activity limitations, or perceived heath. Multimorbidity prevalence varied between 30% (1-year time frame) and 39% (lifetime frame), and more markedly according to sex (higher in women), age (with greatest increases in middle-aged), and socioeconomic status (higher in less educated and low-income individuals and manual workers). We identified various multimorbid combinations, mostly involving vasculometabolic and musculoskeletal conditions and mental disorders, which could be explained by direct causation, shared or associated risk factors, or less frequently, confounding or chance. Combinations with the highest health impacts included diseases with complications but also associations of conditions affecting systems involved in locomotion and sensorial functions (impact on activity limitations), and associations including mental disorders (impact on perceived health). The interaction effects of the associated conditions varied on a continuum from subadditive and additive (associations involving cardiometabolic conditions, low back pain, osteoporosis, injury sequelae, depression, and anxiety) to multiplicative and supermultiplicative (associations involving obesity, chronic obstructive pulmonary disease, migraine, and certain osteoarticular pathologies). Study limitations included self-reported information on chronic conditions and the insufficient power of some analyses.
Conclusions: Multimorbidity assessments should move beyond simply counting conditions and take into account the variable impacts on health status, etiological pathways, and joint effects of associated conditions. In particular, the multimorbid combinations with substantial health impacts or shared risk factors deserve closer attention. Our findings also suggest that multimorbidity assessment and management may be beneficial already in midlife and probably earlier in disadvantaged groups.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- GBD 2017 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392: 1859–922. 10.1016/S0140-6736(18)32335-3 - DOI - PMC - PubMed
-
- van den Akker M, Buntinx F, Knottnerus AJ. Comorbidity or multimorbidity: what’s in a name? A review of literature. Eur J Gen Pract. 1996;2: 65–70.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
