

Lumbar spinal stenosis combined with obesity-induced idiopathic spinal epidural lipomatosis treated with posterior lumbar fusion: case report
- PMID: 33902529
- PMCID: PMC8077912
- DOI: 10.1186/s12893-021-01157-8
Lumbar spinal stenosis combined with obesity-induced idiopathic spinal epidural lipomatosis treated with posterior lumbar fusion: case report
Abstract
Background: Spinal epidural lipomatosis is a rare cause of lumbar spinal stenosis. While conservative therapy is applicable for most of cases, surgical intervention is necessary for severe ones. This is the first time we apply this modified technique to this disease.
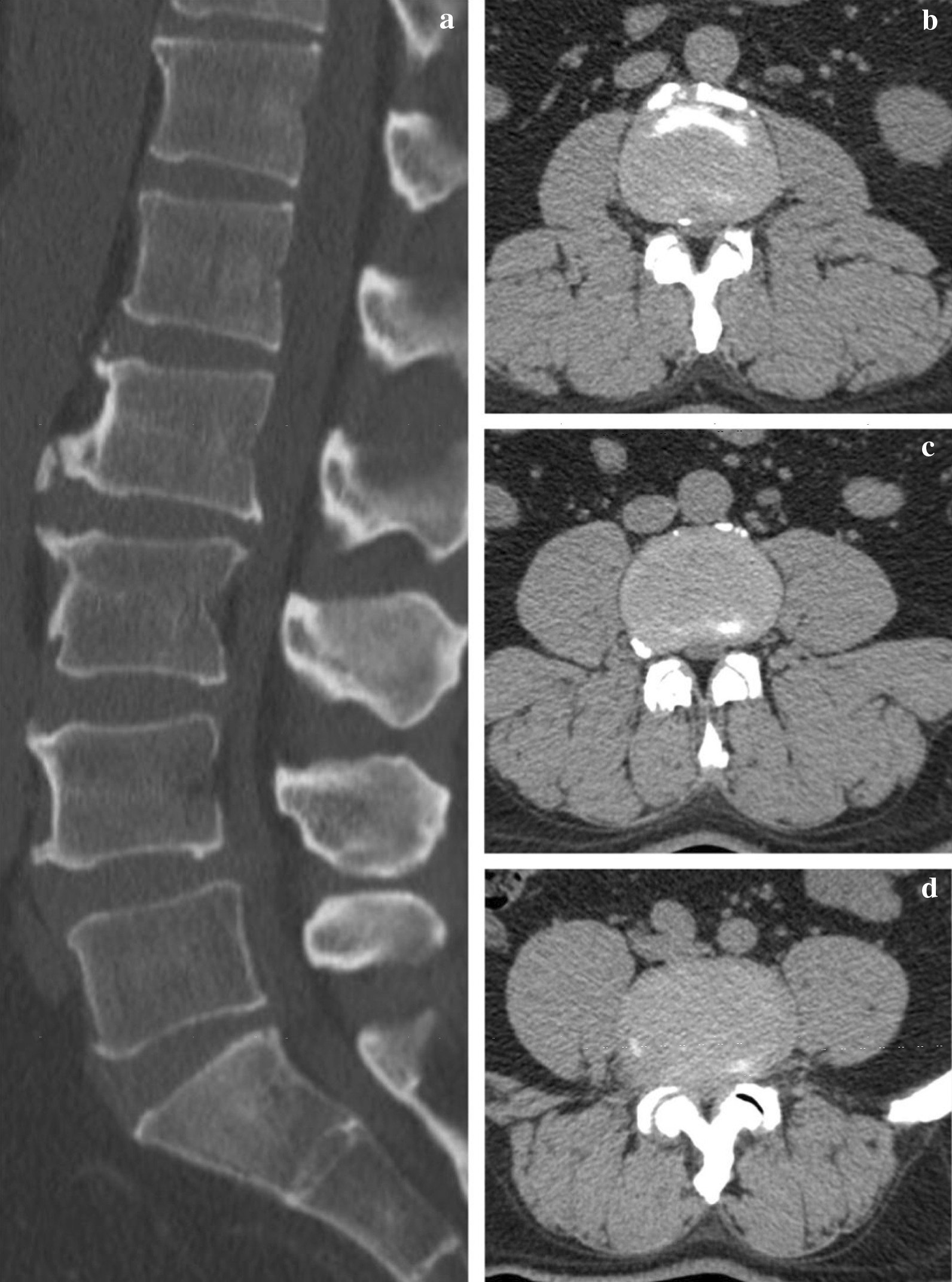
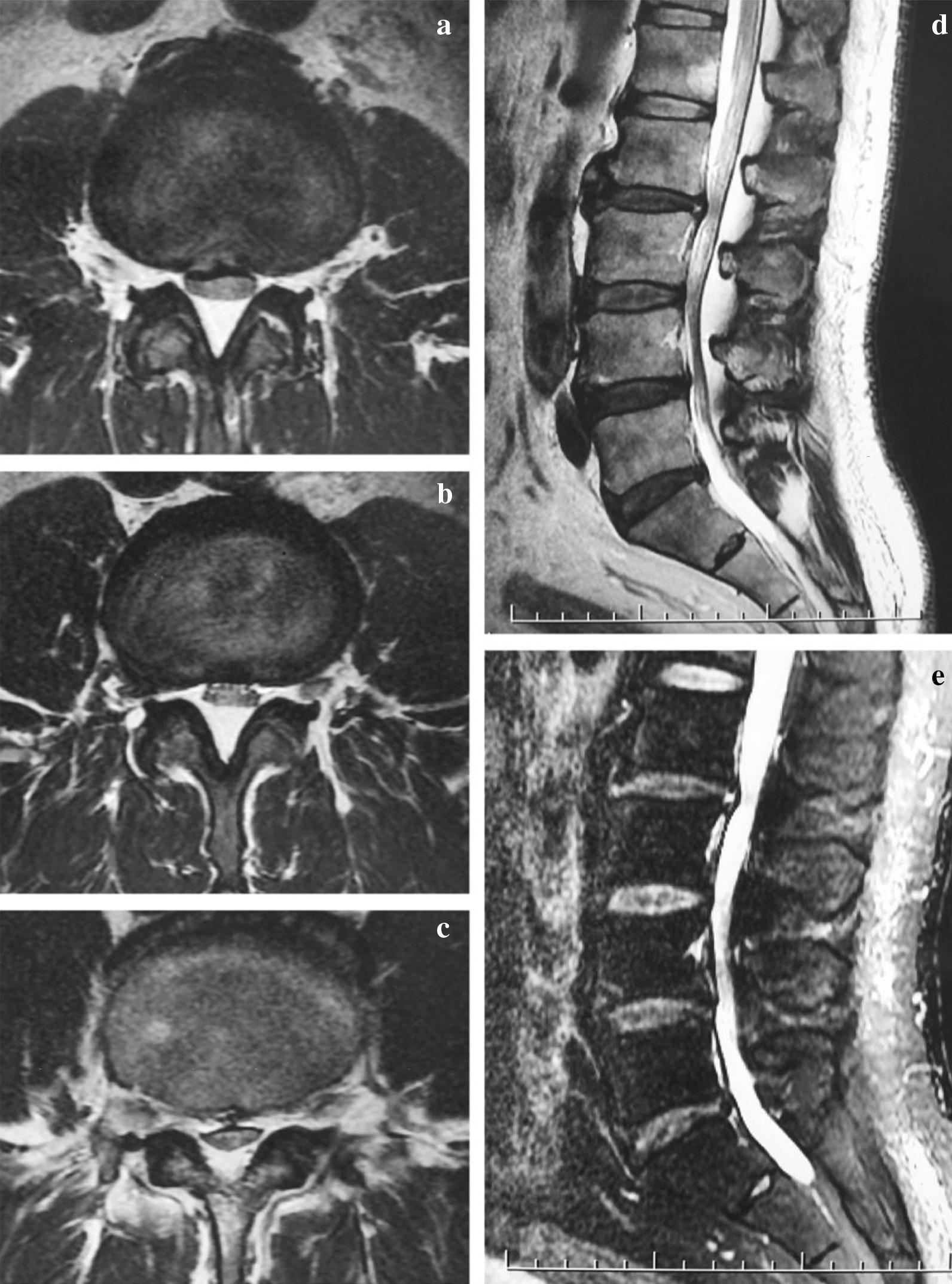
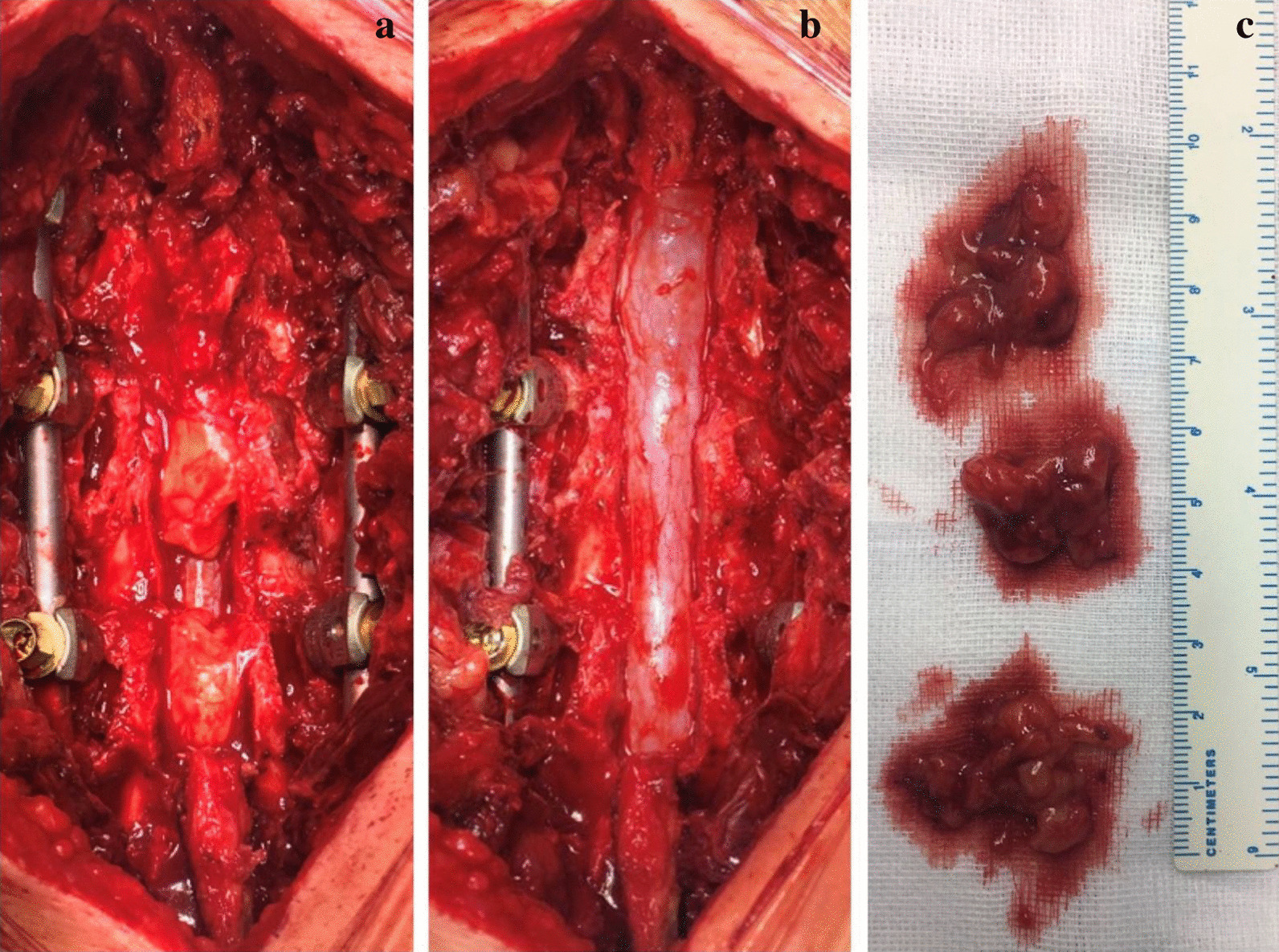
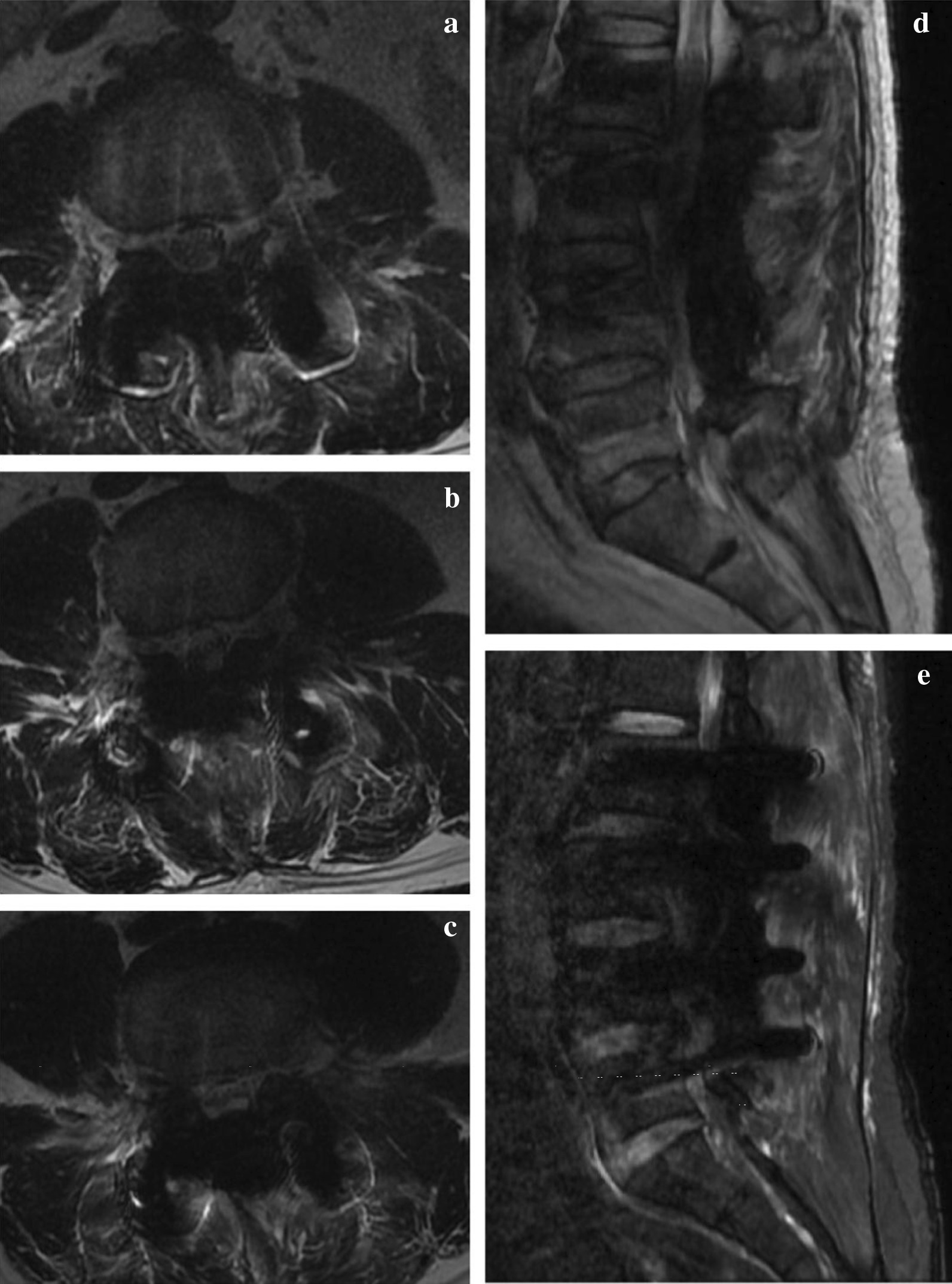
Case presentation: The case is a 53-year-old man. He is 175 cm tall and weighs 102 kg (body mass index 33.3 kg/cm2), presenting with low back pain and bilateral legs pain and numbness. Radiological examination showed severe lumbar spinal stenosis resulting from adipose hyperplasia, combined with hyperosteogeny and hypertrophy of ligaments, which are common etiological factors. Posterior decompression, internal fixation and a modified articular fusion technique was performed on this patient, and regular follow-up that up o 22 months showed outstanding clinical outcomes.
Conclusions: A suitable style of posterior lumbar fusion should be considered to especially severe case with lumbar spinal stenosis and idiopathic spinal epidural lipomatosis.
Keywords: Case report; Lumbar spinal stenosis; Obesity; Posterior lumbar fusion; Spinal epidural lipomatosis.
Conflict of interest statement
All authors declare that they have no competing interests.
Figures



References
-
- Fassett DR, Schmidt MH. Spinal epidural lipomatosis: a review of its causes and recommendations for treatment. Neurosurg Focus. 2004;16(4):E11. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
