

Examining the level and inequality in health insurance coverage in 36 sub-Saharan African countries
- PMID: 33903176
- PMCID: PMC8076950
- DOI: 10.1136/bmjgh-2020-004712
Examining the level and inequality in health insurance coverage in 36 sub-Saharan African countries
Abstract
Introduction: Low/middle-income countries (LMICs) in sub-Saharan Africa (SSA) are increasingly turning to public contributory health insurance as a mechanism for removing financial barriers to access and extending financial risk protection to the population. Against this backdrop, we assessed the level and inequality of population coverage of existing health insurance schemes in 36 SSA countries.
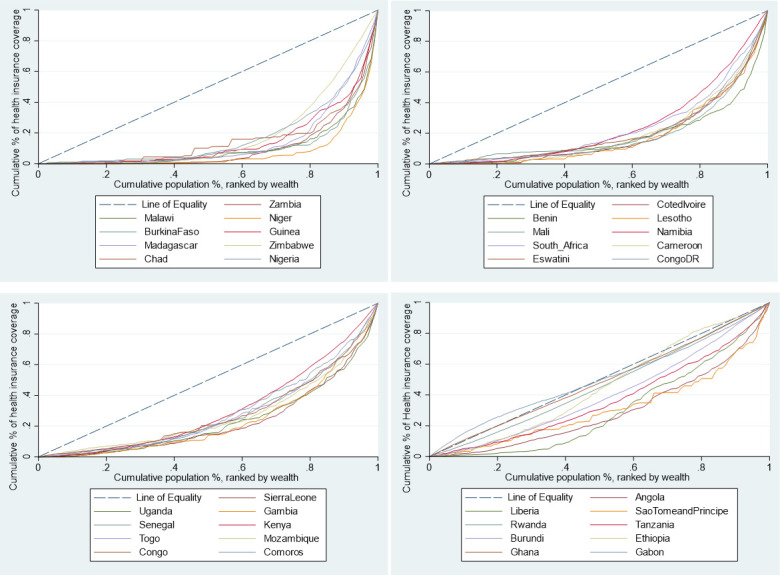
Methods: Using secondary data from the most recent Demographic and Health Surveys, we computed mean population coverage for any type of health insurance, and for specific forms of health insurance schemes, by country. We developed concentration curves, computed concentration indices, and rich-poor differences and ratios to examine inequality in health insurance coverage. We decomposed the concentration index using a generalised linear model to examine the contribution of household and individual-level factors to the inequality in health insurance coverage.
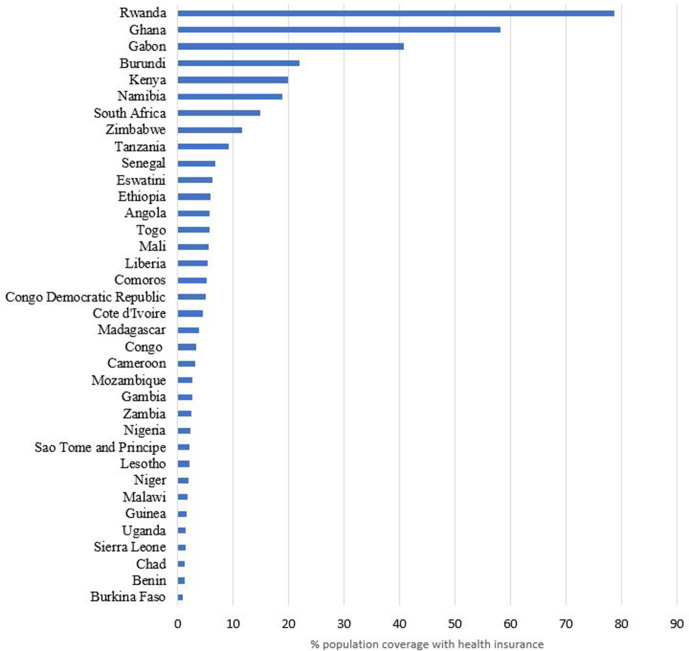
Results: Only four countries had coverage levels with any type of health insurance of above 20% (Rwanda-78.7% (95% CI 77.5% to 79.9%), Ghana-58.2% (95% CI 56.2% to 60.1%), Gabon-40.8% (95% CI 38.2% to 43.5%), and Burundi 22.0% (95% CI 20.7% to 23.2%)). Overall, health insurance coverage was low (7.9% (95% CI 7.8% to 7.9%)) and pro-rich; concentration index=0.4 (95% CI 0.3 to 0.4, p<0.001). Exposure to media made the greatest contribution to the pro-rich distribution of health insurance coverage (50.3%), followed by socioeconomic status (44.3%) and the level of education (41.6%).
Conclusion: Coverage of health insurance in SSA is low and pro-rich. The four countries that had health insurance coverage levels greater than 20% were all characterised by substantial funding from tax revenues. The other study countries featured predominantly voluntary mechanisms. In a context of high informality of labour markets, SSA and other LMICs should rethink the role of voluntary contributory health insurance and instead embrace tax funding as a sustainable and feasible mechanism for mobilising resources for the health sector.
Keywords: health economics; health insurance; health systems.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- global forum for health research Geneva . Learning from experience: health care financing in low-and middle-income countries 2007.
-
- Gottret P, Schieber G. Health financing revisited: a practitioner’s guide: The World Bank 2006.
-
- Organization WH . The world health report: 2004: changing history: World Health organization 2004.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials