

Systemic and organ-specific immune-related manifestations of COVID-19
- PMID: 33903743
- PMCID: PMC8072739
- DOI: 10.1038/s41584-021-00608-z
Systemic and organ-specific immune-related manifestations of COVID-19
Abstract
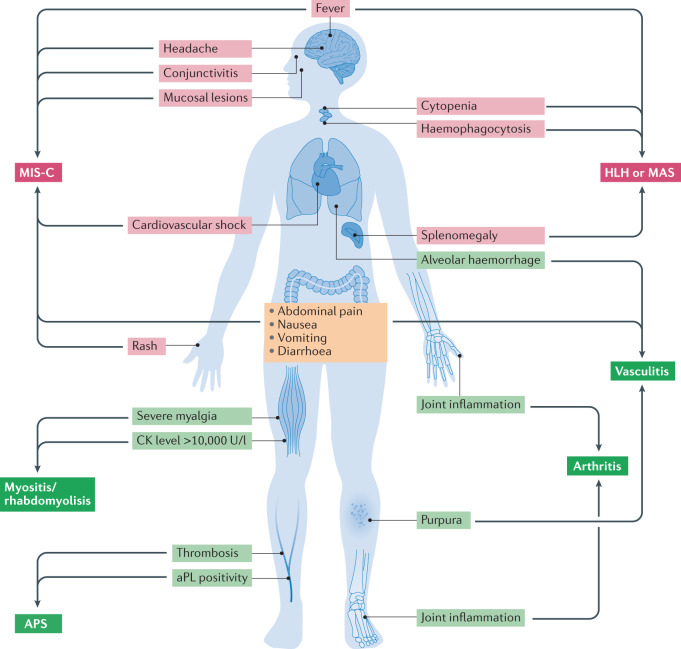
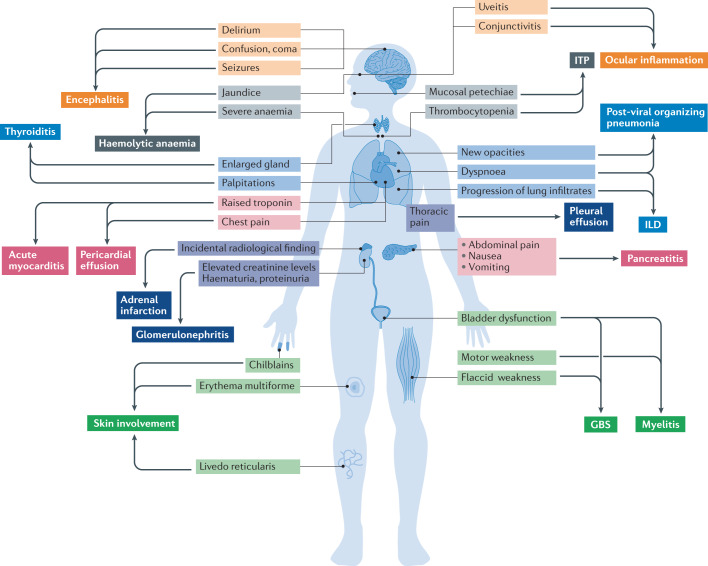
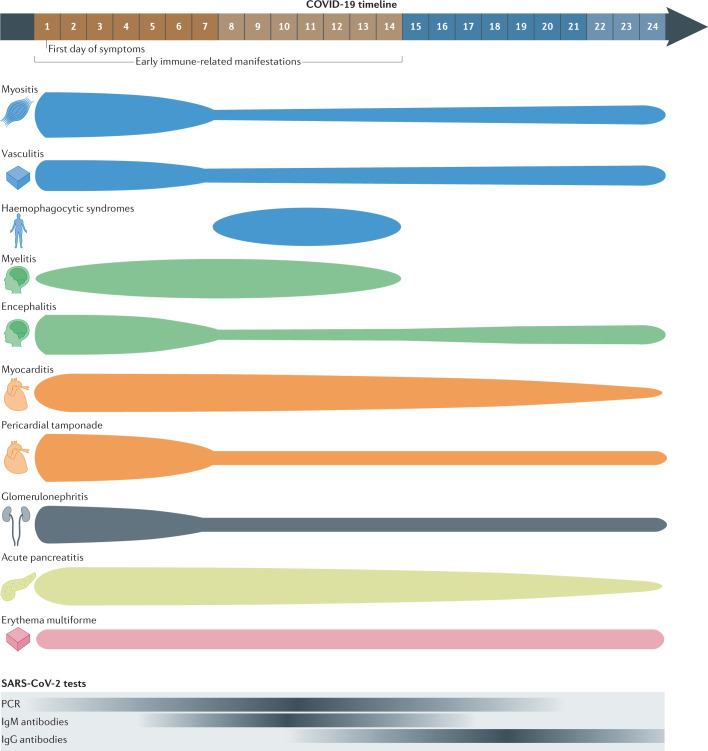
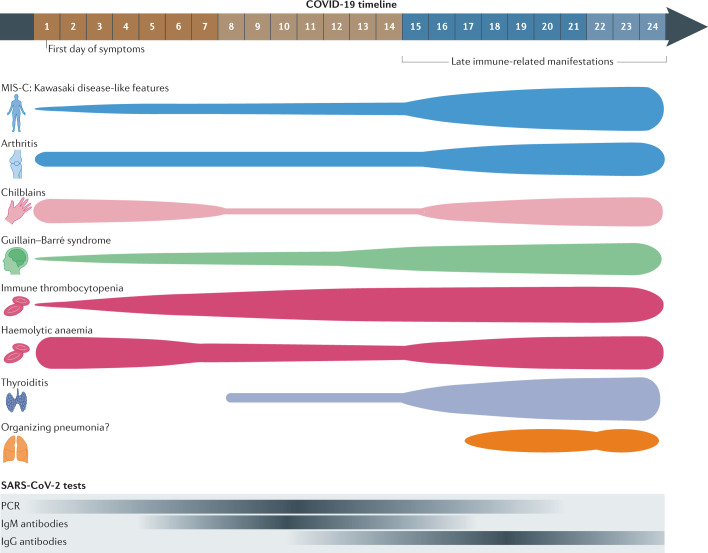
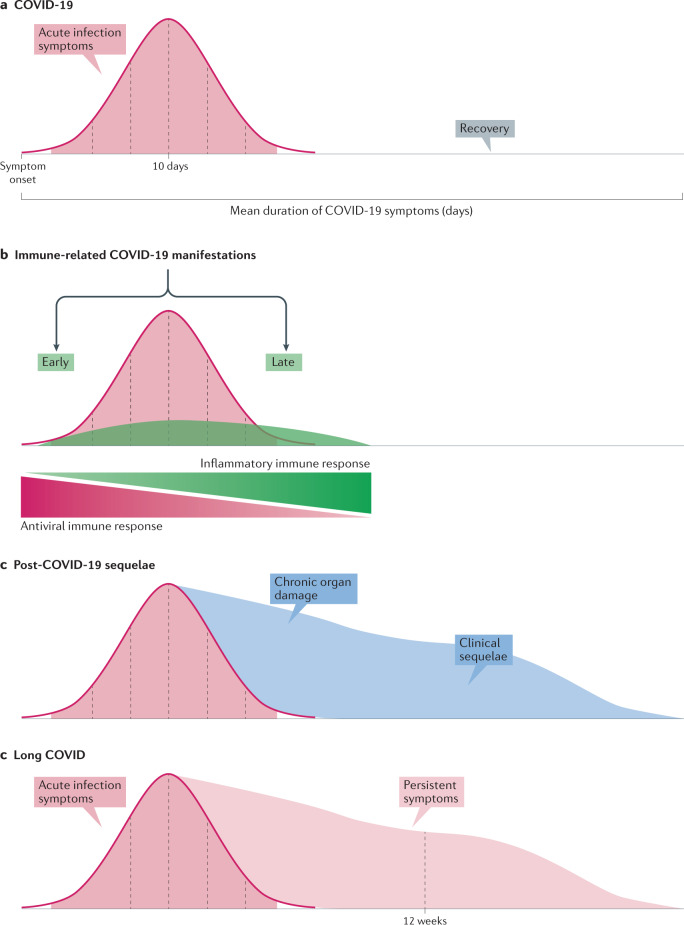
Immune-related manifestations are increasingly recognized conditions in patients with COVID-19, with around 3,000 cases reported worldwide comprising more than 70 different systemic and organ-specific disorders. Although the inflammation caused by SARS-CoV-2 infection is predominantly centred on the respiratory system, some patients can develop an abnormal inflammatory reaction involving extrapulmonary tissues. The signs and symptoms associated with this excessive immune response are very diverse and can resemble some autoimmune or inflammatory diseases, with the clinical phenotype that is seemingly influenced by epidemiological factors such as age, sex or ethnicity. The severity of the manifestations is also very varied, ranging from benign and self-limiting features to life-threatening systemic syndromes. Little is known about the pathogenesis of these manifestations, and some tend to emerge within the first 2 weeks of SARS-CoV-2 infection, whereas others tend to appear in a late post-infectious stage or even in asymptomatic patients. As the body of evidence comprises predominantly case series and uncontrolled studies, diagnostic and therapeutic decision-making is unsurprisingly often based on the scarcely reported experience and expert opinion. Additional studies are required to learn about the mechanisms involved in the development of these manifestations and apply that knowledge to achieve early diagnosis and the most suitable therapy.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Wiersinga WJ, Rhodes A, Cheng AC, Peacock SJ, Prescott HC. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): a review. JAMA. 2020;324:782–793. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
